Case Western Reserve University / MetroHealth Cleveland, OH
Award: ACG Presidential Poster Award
Josue A. Davila, MD, Sherif Saleh, MD, Nisheet Waghray, MD Case Western Reserve University / MetroHealth, Cleveland, OH Introduction: Russell body duodenitis (RBD) is a rare plasma cell-rich inflammatory condition defined by Mott cells containing eosinophilic immunoglobulin inclusions known as Russell bodies. Though most commonly described in the gastric mucosa, duodenal involvement is exceedingly rare and may mimic neoplastic processes. Recognition of this benign entity is essential to avoid unnecessary interventions.
Case Description/
Methods: A 60-year-old male with a history of alcohol and tobacco use, atrial fibrillation on apixaban, coronary artery disease, and peripheral arterial disease presented with melena and chronic anemia. He was pale but hemodynamically stable. Laboratory evaluation revealed a hemoglobin of 9.8 g/dL and elevated pro-BNP. Esophagogastroduodenoscopy showed an edematous, nodular duodenal bulb without active bleeding, along with diffuse gastritis and moderate portal hypertensive gastropathy. Duodenal biopsies were obtained.
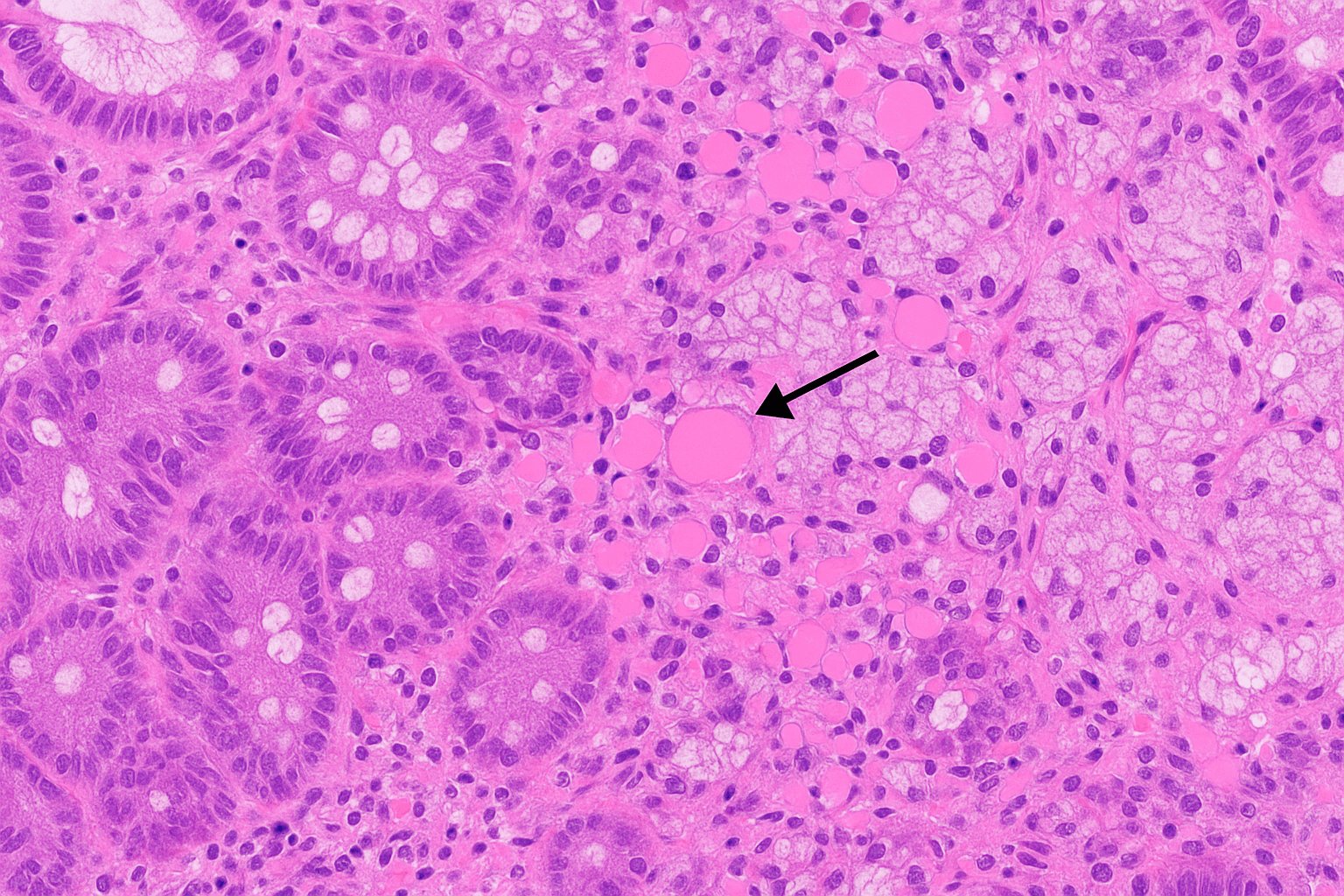
Histologic analysis revealed preserved villous architecture with chronic inflammation and numerous Mott cells containing eosinophilic Russell bodies. Immunohistochemistry showed CD138-positive plasma cells with polytypic kappa and lambda light chain expression. Special stains for Helicobacter pylori and D2-40 were negative. There was no evidence of HIV, autoimmune disease, or gastrointestinal malignancy. The patient improved with supportive care and was discharged in stable condition. Discussion: Fewer than ten published cases of RBD have been reported. Proposed mechanisms include chronic antigenic stimulation, endoplasmic reticulum (ER) stress impairing immunoglobulin secretion, and altered plasma cell differentiation. Although rare associations with malignancies have been documented, these appear incidental. Histologic evaluation, particularly with immunohistochemical staining for CD138 and light chains, is critical to distinguish RBD from plasma cell neoplasms and avoid unnecessary oncologic workup. This case reinforces the importance of including RBD in the differential diagnosis of nodular duodenal lesions, particularly in patients with upper GI symptoms and chronic mucosal changes.
Figure: Histologic section of the duodenal mucosa demonstrating numerous Mott cells (plasma cells with intracytoplasmic Russell bodies) in the lamina propria. Arrow indicates a representative Russell body, characterized by its eosinophilic, globular appearance.
Figure: Endoscopic image of the duodenal bulb showing nodular and edematous mucosa. Arrow indicates the most prominently raised area, which was biopsied and later confirmed to show Russell body duodenitis.
Disclosures: Josue Davila indicated no relevant financial relationships. Sherif Saleh indicated no relevant financial relationships. Nisheet Waghray indicated no relevant financial relationships.
Josue A. Davila, MD, Sherif Saleh, MD, Nisheet Waghray, MD. P2008 - Russell Body Duodenitis in a 60-Year-Old Male With Upper Gastrointestinal Bleeding: A Rare Mimicker of Malignancy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.