Dayanand Medical College and Hospital Jalandhar, Punjab, India
Ramit Mahajan, MBBS, MD, DM1, Fnu Bhawna, MBBS2, Rubina Khullar Mahajan, MD1, Chandan Kakkar, MD1, Ajit Sood, DM1, Ashvind Bawa, MS1, Bishav Mohan, DM1, Aminder Singh, MD1 1Dayanand Medical College and Hospital, Ludhiana, Punjab, India; 2Dayanand Medical College and Hospital, Jalandhar, Punjab, India Introduction: Chronic Atrial and Intestinal Dysrhythmia (CAID) syndrome is a rare autosomal recessive disorder characterized by chronic intestinal pseudo-obstruction (CIPO) and cardiac conduction abnormalities, most often bradyarrhythmias. It is commonly associated with pathogenic variants in the SGOL1 gene, which disrupts chromosomal cohesion in rapidly dividing tissues like the gastrointestinal tract and cardiac conduction system. Fewer than 30 cases have been reported globally since its first description in 2014, making each new report critical to understanding this rare disorder.
Case Description/
Methods: We report two familial cases of CAID syndrome from an endogamous North Indian community.
Case 1: A 16-year-old female presented with progressive abdominal distension, constipation, bradycardia, and syncopal episodes. Imaging showed intestinal dilatation without obstruction. Despite prokinetics and later surgical intervention, her condition deteriorated, and she succumbed to severe intestinal dysmotility and malnutrition.
Case 2: Her 17-year-old male cousin presented five years later with similar symptoms. Exploratory laparotomy ruled out mechanical obstruction. ECG showed bradycardia and first-degree AV block. Genetic testing confirmed a homozygous SGOL1 mutation (c.67A >G, p.Lys23Glu), establishing the diagnosis of CAID. He responded to prokinetics and a temporary ileostomy, followed by successful reversal and clinical stabilization. Discussion: Our experience underscores the need for early genetic testing in patients with unexplained pseudo-obstruction and arrhythmia. While gastrointestinal symptoms often precede cardiac findings, bradyarrhythmias may be underrecognized. The surgical intervention had different outcomes in the two cases, highlighting the need for careful patient selection and risk-benefit evaluation before surgery. Nutritional support is pivotal, as malnutrition remains a key cause of mortality. Interdisciplinary collaboration among gastroenterologists, cardiologists, geneticists, surgeons, and nutritionists is vital, along with referral to specialized motility disorder centers. Larger cohort studies are urgently needed to define genotype-phenotype correlations and biomarkers of disease progression. There is also a critical need to evaluate prokinetic drugs, cardiac pacing, and molecular therapies systematically. Clinicians should consider CAID in young patients presenting with pseudo-obstruction and arrhythmias, enabling timely diagnosis, genetic counseling, and tailored management.
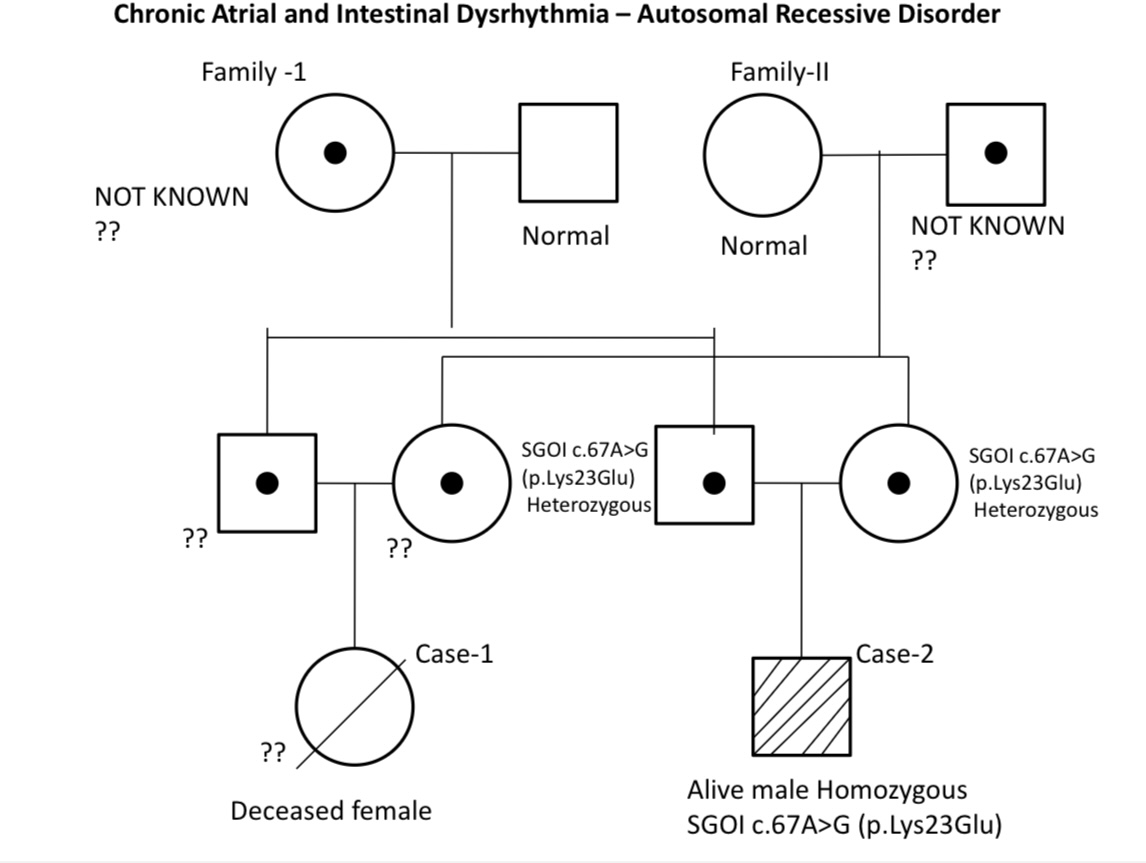
Figure: Pedigree demonstrating autosomal recessive inheritance of CAID syndrome due to a homozygous SGOL1 (c.67A>G; p.Lys23Glu) mutation. The affected individuals (Case 1: deceased female; Case 2: alive male) are double first cousins born to siblings from both paternal and maternal sides, each carrying a heterozygous pathogenic SGOL1 variant.
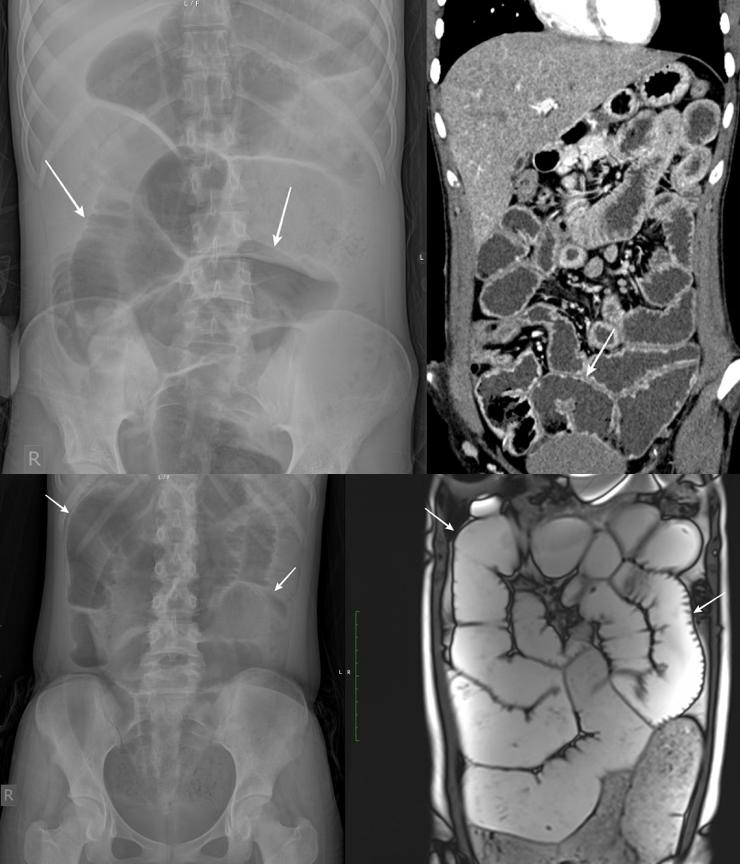
Figure: The above image is of Case 2 and the below image is of Case 1. Case 1: Supine radiograph of the abdomen reveals dilatation of the small bowel loops (arrows). MR enterography image reveals similar dilatation of the small bowel loops (arrows). Case 2: Supine radiograph of the abdomen reveals massive dilatation of the small bowel loops. CT enterography after decompression reveals persistent dilatation of the small bowel loops.
Disclosures: Ramit Mahajan indicated no relevant financial relationships. Fnu Bhawna indicated no relevant financial relationships. Rubina Khullar Mahajan indicated no relevant financial relationships. Chandan Kakkar indicated no relevant financial relationships. Ajit Sood indicated no relevant financial relationships. Ashvind Bawa indicated no relevant financial relationships. Bishav Mohan indicated no relevant financial relationships. Aminder Singh indicated no relevant financial relationships.
Ramit Mahajan, MBBS, MD, DM1, Fnu Bhawna, MBBS2, Rubina Khullar Mahajan, MD1, Chandan Kakkar, MD1, Ajit Sood, DM1, Ashvind Bawa, MS1, Bishav Mohan, DM1, Aminder Singh, MD1. P2007 - When Heart and Gut Rhythms Falter: A Family's Battle with CAID (Chronic Atrial and Intestinal Dysrhythmia) Syndrome, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")