Erin Hollis, DO1, Lauren Davis, DO1, Mark McGarrey, MD1, Julianna Tantum, DO1, Thomas McKenna, MD2 1Lankenau Medical Center, Wynnewood, PA; 2Bryn Mawr, Bryn Mawr, PA Introduction: The differential diagnosis for patients presenting with nausea, vomiting, and abdominal pain is broad, with etiologies ranging from relatively benign conditions to aggressive malignancies. We describe a patient presenting with symptoms of gastric outlet obstruction (GOO) and found to have a malignant stricture due to duodenal adenocarcinoma.
Case Description/
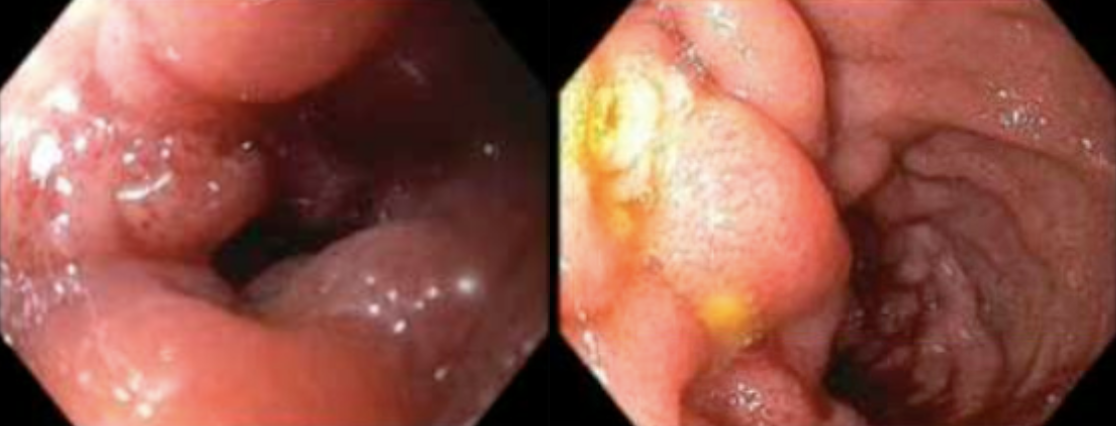
Methods: A 51-year-old male presented to the ED for nausea, vomiting, and left upper quadrant pain. CT of the abdomen/pelvis showed a dilated stomach and duodenum with wall irregularity and inflammation of the duodenum. He was treated with NG tube decompression and underwent EGD which revealed diffuse severe erythema and friability in the third portion of the duodenum; the area was traversed with a neonatal scope revealing a normal D4. Pathology showed chronic duodenitis. The patient tolerated a diet and was discharged with the plan for repeat EGD in one month. He presented back to the hospital 8 days later with continued symptoms. Repeat EGD was done showing edematous mucosa in the second portion of the duodenum with severe stenosis that was partially traversed with a neonatal scope revealing an area of ulcerated oozing mucosa (Figure). Pathology was concerning for adenocarcinoma. The patient was initiated on TPN and underwent repeat EGD with advanced GI and a duodenal stent was placed. Patient ultimately underwent pylorus preserving pancreaticoduodenectomy. Pathology confirmed invasive adenocarcinoma of the duodenum, invading into the pancreas. The patient was initiated on folinic acid, fluorouracil, and oxaliplatin (FOLFOX), and after three cycles, bevacizumab was added to his regimen. Interval CT imaging has shown positive response to therapy. Discussion: Malignancy of the small intestine is rare, accounting for less than five percent of all gastrointestinal (GI) malignancies. Adenocarcinoma of the small intestine accounts for only one percent of all GI malignancies, and often presents with nonspecific signs and symptoms, frequently leading to a delay in diagnosis. This case underscores the importance of having adequate clinical suspicion to carry out the necessary radiographic and endoscopic diagnostics in order to determine the underlying etiology. This case also highlights how repeated presentations and endoscopies may be necessary to finally elucidate the underlying cause, as GOOs can cause waxing and waning and nonspecific symptoms.
Figure: Endoscopic images of friable edematous mucosa in the second portion of the duodenum
Disclosures: Erin Hollis indicated no relevant financial relationships. Lauren Davis indicated no relevant financial relationships. Mark McGarrey indicated no relevant financial relationships. Julianna Tantum indicated no relevant financial relationships. Thomas McKenna indicated no relevant financial relationships.
Erin Hollis, DO1, Lauren Davis, DO1, Mark McGarrey, MD1, Julianna Tantum, DO1, Thomas McKenna, MD2. P2002 - An Uncommon Cause of a Common Symptom: Duodenal Adenocarcinoma Presenting With Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.