NYC Health + Hospitals/Woodhull Brooklyn, San Salvador, El Salvador
Gulce Karaca, MD1, Ana Maritza Marulanda Prado, MD1, Julio C. Valencia, MD2, Beishi Zheng, MD2, Dalia Mahmoud Hassan Elamin, MD1 1NYC Health + Hospitals/Woodhull, Brooklyn, NY; 2NYC Health + Hospitals/Metropolitan, New York, NY Introduction: IgG4-related disease (IgG4-RD) is a rare, slowly progressive fibroinflammatory disorder that can affect multiple organs. Its diagnosis is often challenging, as clinical and radiologic features may mimic other conditions. In the gastrointestinal tract, it frequently resembles cholangiocarcinoma or pancreatic cancer. We present a case of IgG4-related sclerosing cholangitis (IgG4-SC) with autoimmune pancreatitis (AIP) mimicking cholangiocarcinoma.
Case Description/
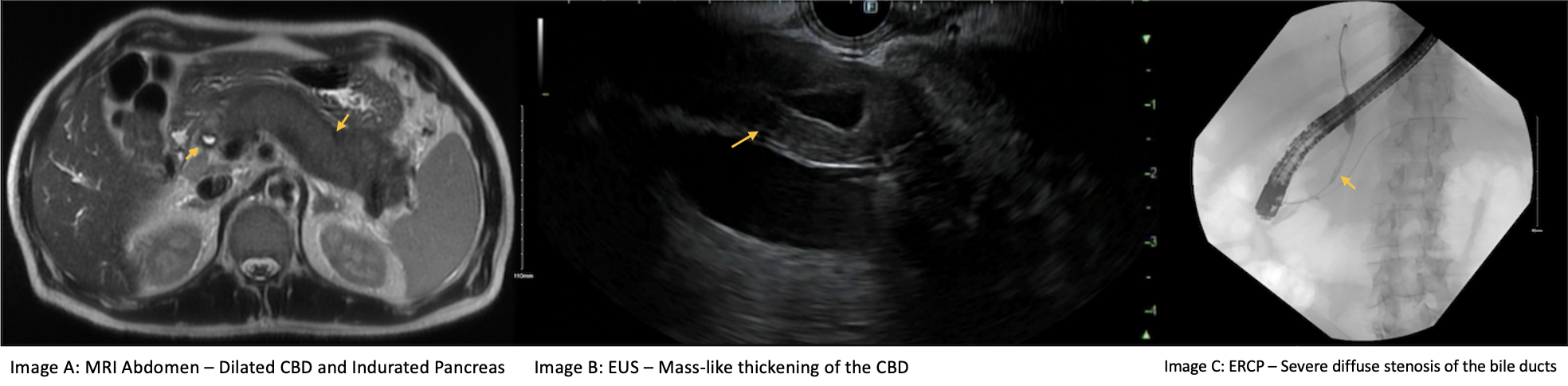
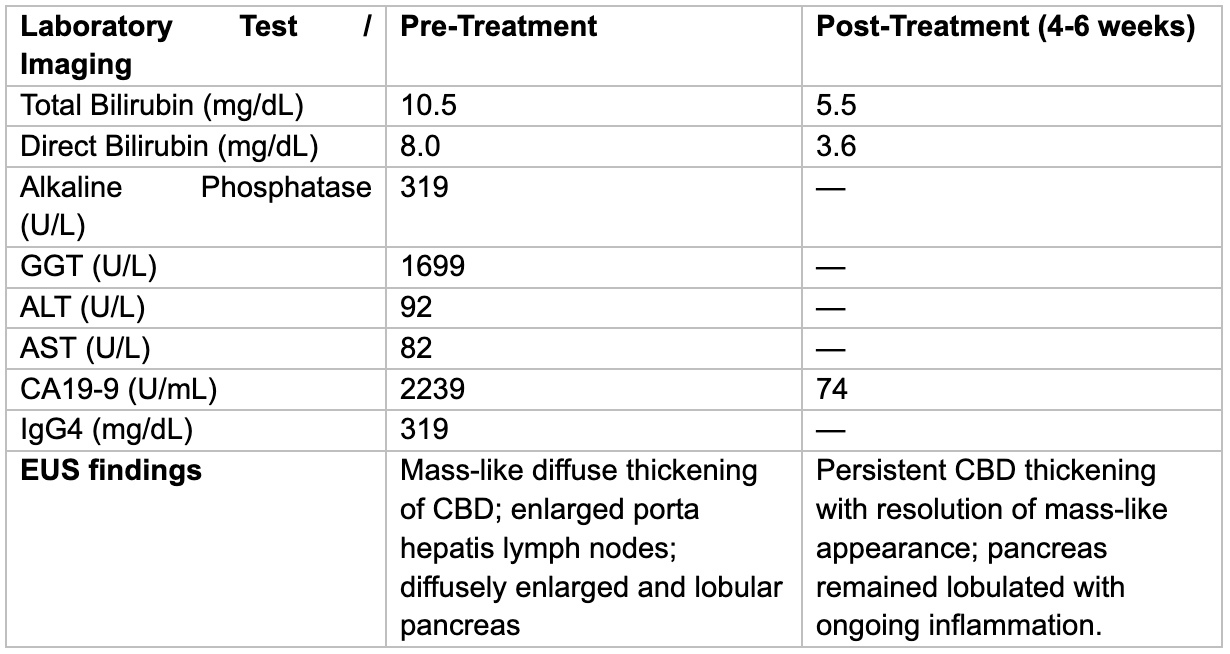
Methods: A 73-year-old man presented with progressive jaundice, abdominal pain, acholia, choluria, and a 40-pound weight loss over four months. Physical exam was notable for jaundice and epigastric tenderness. Initial workup revealed cholestatic liver enzyme elevation, and the ultrasound showed a 1.3 cm CBD, intrahepatic ductal dilation, and heterogeneous pancreatic texture. Following MRCP confirmed diffuse pancreatic induration and biliary dilation. EUS revealed mass-like thickening of the CBD and enlarged porta hepatis nodes. ERCP showed multiple strictures; FNA from the CBD and nodes was negative for malignancy. Despite features concerning for malignancy, including CA19-9 of 2239 U/mL, elevated IgG4 (319 mg/dL) keeping IgG4-RD high in the differential, and prednisone 40 mg daily was initiated. The patient responded clinically with significant biochemical improvement, including reduction of CA19-9. On repeat EUS, the CBD mass resolved, and FNA again showed no malignancy. The pancreas remained lobulated and enlarged; biopsy revealed chronic pancreatitis with lymphoplasmacytic infiltrate and up to 18 IgG4+ plasma cells/hpf, confirming IgG4-RD. Discussion: IgG4-RD is a multisystem, immune-mediated disease with nonspecific symptoms and insidious onset, often mimicking malignancy. Its presentation may resemble pancreatic cancer, PSC, or cholangiocarcinoma. Our patient had features of IgG4-SC with AIP, including pancreatic enlargement, biliary strictures, and steroid response, but also findings concerning for malignancy, such as mass-like CBD thickening and CA19-9 >2000. The HISORt criteria guide diagnosis based on histology, imaging, serology, other organ involvement, and response to therapy. Serum IgG4 > 300 mg/dL and elevated bile IgG4 levels can help distinguish IgG4-SC from cancer. CA19-9 < 85 U/mL has been proposed to support AIP over malignancy, and normalization after treatment in our case further favored a benign etiology. Recognition of overlapping features is critical to avoid misdiagnosis and unnecessary surgical intervention.
Figure: Image A. CT abdomen - EUS - ERCP images
Figure: Table 1. Laboratory and EUS findings pre- and 4–6 weeks post-treatment.
Disclosures: Gulce Karaca indicated no relevant financial relationships. Ana Maritza Marulanda Prado indicated no relevant financial relationships. Julio C. Valencia indicated no relevant financial relationships. Beishi Zheng indicated no relevant financial relationships. Dalia Mahmoud Hassan Elamin indicated no relevant financial relationships.
Gulce Karaca, MD1, Ana Maritza Marulanda Prado, MD1, Julio C. Valencia, MD2, Beishi Zheng, MD2, Dalia Mahmoud Hassan Elamin, MD1. P2252 - A Case of IgG4-related Cholangiopathy and Pancreatopathy Mimicking Cholangiocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")