University of Rochester Medical Center Rochester, NY
Junseo Lee, MD, Ashwath Elangovan, , Joshua Rosario, , Philomena Burger, BA, Truptesh H. Kothari, MD, MS, FACG University of Rochester Medical Center, Rochester, NY Introduction: Lemmel Syndrome (LS) is a rare cause of obstructive jaundice, resulting from a large peri-ampullary duodenal diverticulum causing compression of the common bile duct (CBD), in the absence of a mass or choledocholithiasis. Although duodenal diverticula are common and often incidental findings, they infrequently cause complications, making LS a diagnostic and management challenge. With advancements in endoscopic imaging and therapeutic techniques, the recognition and management of LS are evolving. We present a case series highlighting its importance in the evaluation of biliary obstruction and outlining the difference in management strategies.
Case Description/
Methods: First is a 78 M with esophageal strictures, hiatal hernia, and Lynch syndrome who presented with abdominal pain and imaging with biliary dilation. MRCP revealed a large periampullary duodenal diverticulum compressing the CBD. Blood cultures grew K. pneumoniae and E. coli. He was treated with Zosyn and cholecystectomy (CCY). He recovered well and was discharged on oral antibiotics. Second, an 85 M with GERD, complicated cholecystitis, and prior sphincterotomy presented with fever, nausea, and confusion. Labs revealed transaminitis and CBD dilation on ultrasound. Blood cultures grew Klebsiella, and he was treated with Zosyn. ERCP revealed both a duodenal and periampullary diverticulum with a bile duct stricture. The duct was swept and nothing was found. The CBD was stented, and the patient recovered well with normalization of LFTs. Last, a 72 F with prior CCY presented with recurrent right upper quadrant abdominal pain and pale stools. Imaging revealed progressive biliary and PD dilation and a large periampullary diverticulum. LFTs were elevated including lipase. After a failed initial ERCP due to obscured anatomy, EUS confirmed extrinsic compression consistent with LS. A repeat ERCP with CBD and PD stenting was successfully performed. On imaging, none of the patients had a pancreas mass. Discussion: The cases highlight the unique presentations of LS and the pivotal role of endoscopic techniques, particularly ERCP, in both diagnosis and treatment. In one case, distorted anatomy required EUS, underscoring its value when ERCP is limited. While two cases were managed with biliary stenting, one patient underwent CCY, emphasizing the need for individualized strategies based on anatomy and clinical course. Literature supports ERCP with sphincterotomy and stenting as first-line therapy, reserving surgery for refractory or recurrent cases.
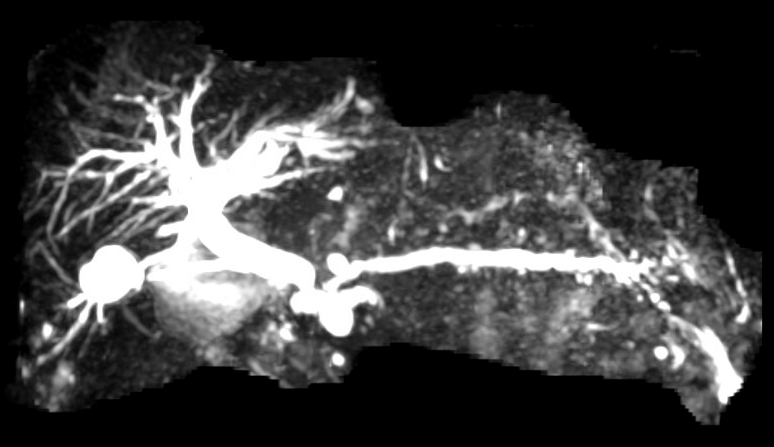
Figure: MRCP demonstrating a CBD stricture with proximal extrahepatic duct dilation as well as PD dilation and stricture.
Figure: ERCP showing a large duodenal diverticulum with ampulla noted inside a small diverticulum. A plastic CBD stent was placed.
Disclosures: Junseo Lee indicated no relevant financial relationships. Ashwath Elangovan indicated no relevant financial relationships. Joshua Rosario indicated no relevant financial relationships. Philomena Burger indicated no relevant financial relationships. Truptesh Kothari indicated no relevant financial relationships.
Junseo Lee, MD, Ashwath Elangovan, , Joshua Rosario, , Philomena Burger, BA, Truptesh H. Kothari, MD, MS, FACG. P2248 - Lemmel Syndrome: A Case Series of Duodenal Diverticula Causing Obstructive Jaundice, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Junseo Lee, MD (he/him/his) photo")