Hamza Khan, MD1, Muhammad Qasim Chaudhry, MD2, Mark Kwarciak, MD3, Kunal Deora, MD1 1Midwestern University, Cottonwood, AZ; 2Landmark Medical Center, Cumberland, RI; 3NORTHERN ARIZONA HEALTHCARE, Flagstaff, AZ Introduction: Periampullary diverticula are found in up to 20% of patients undergoing ERCP but are rarely implicated in clinical pathology. While commonly asymptomatic, they may occasionally lead to pancreaticobiliary complications such as cholangitis or, more rarely, acute pancreatitis. This case highlights duodenal diverticulitis as an underrecognized etiology of pancreatitis and cholestatic liver injury, particularly in the absence of traditional risk factors.
Case Description/
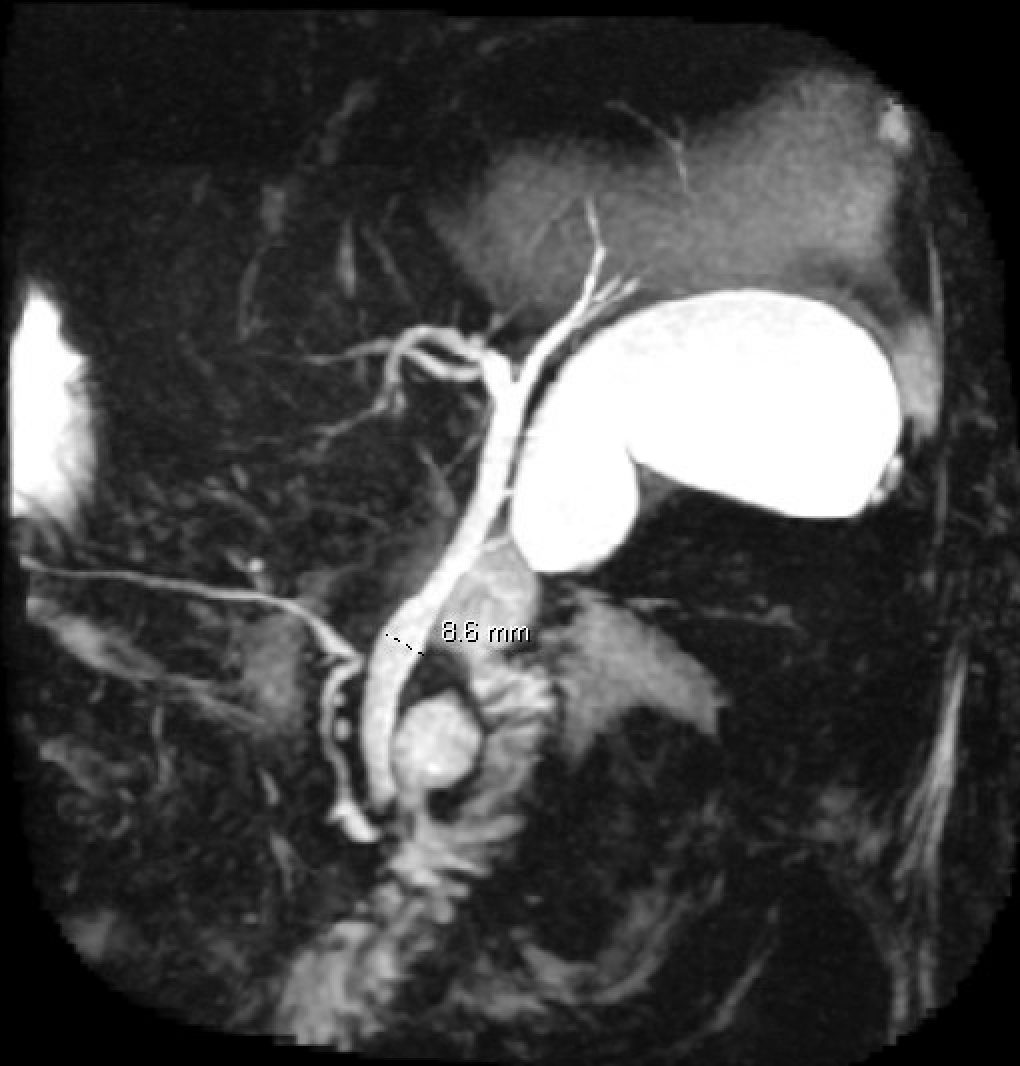
Methods: An 82-year-old female with a medical history of atrial fibrillation, coronary artery disease, and hypertension presented with acute epigastric pain. Initial workup showed mild lipase elevation (69 U/L), leukocytosis, CRP 91 mg/L, procalcitonin 52.15 ng/mL, and transaminitis (ALT 473 U/L, AST 835 U/L) with hyperbilirubinemia (peak 3.3 mg/dL). CT abdomen confirmed acute pancreatitis. Abdominal ultrasound showed no cholelithiasis or cholecystitis. MRCP revealed an 8 mm dilated common bile duct and a large periampullary duodenal diverticulum without obstructive stones. Surgical review and radiological correlation concluded that diverticulitis was the likely cause of pancreatitis and biliary obstruction. ERCP was deferred due to absence of definitive obstruction. The patient was managed with moderately aggressive fluid resuscitation for pancreatitis and conservative management was employed with IV antibiotics for diverticulitis with eventual clinical resolution. No further intervention was deemed necessary.
Discussion: Duodenal diverticula are common incidental findings, yet they may rarely cause acute pancreatitis through mechanical or inflammatory compromise of the ampulla or pancreaticobiliary outflow. In this case, absence of gallstones or alcohol use, combined with imaging and clinical improvement on antibiotics, implicated diverticulitis as the etiology. Recognition of this rare association is critical, particularly in elderly patients with idiopathic pancreatitis. Conservative management may be sufficient, though endoscopic or surgical approaches may be warranted in select cases. Close follow-up is essential given the potential for recurrence.
Figure: Duodenal Diverticulum leading to an obstructive cause of acute pancreatitis
Disclosures: Hamza Khan indicated no relevant financial relationships. Muhammad Qasim Chaudhry indicated no relevant financial relationships. Mark Kwarciak indicated no relevant financial relationships. Kunal Deora indicated no relevant financial relationships.
Hamza Khan, MD1, Muhammad Qasim Chaudhry, MD2, Mark Kwarciak, MD3, Kunal Deora, MD1. P2242 - An Unusual Culprit: Duodenal Diverticulitis as the Cause of Acute Pancreatitis and Cholestasis in an Elderly Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.