David Guevara-Lazo, MD, Jonathan B.. McHugh, MD, Jorge D.. Machicado, MD, MPH University of Michigan, Ann Arbor, MI Introduction: Among all pancreatic and peripancreatic tumors, pancreatic cancer is usually the most common cause. However, a number of other tumors, even with an indolent course can occur in the pancreas and its vicinity. In this case, we report a patient with a peripancreatic tumor of an unexpected etiology.
Case Description/
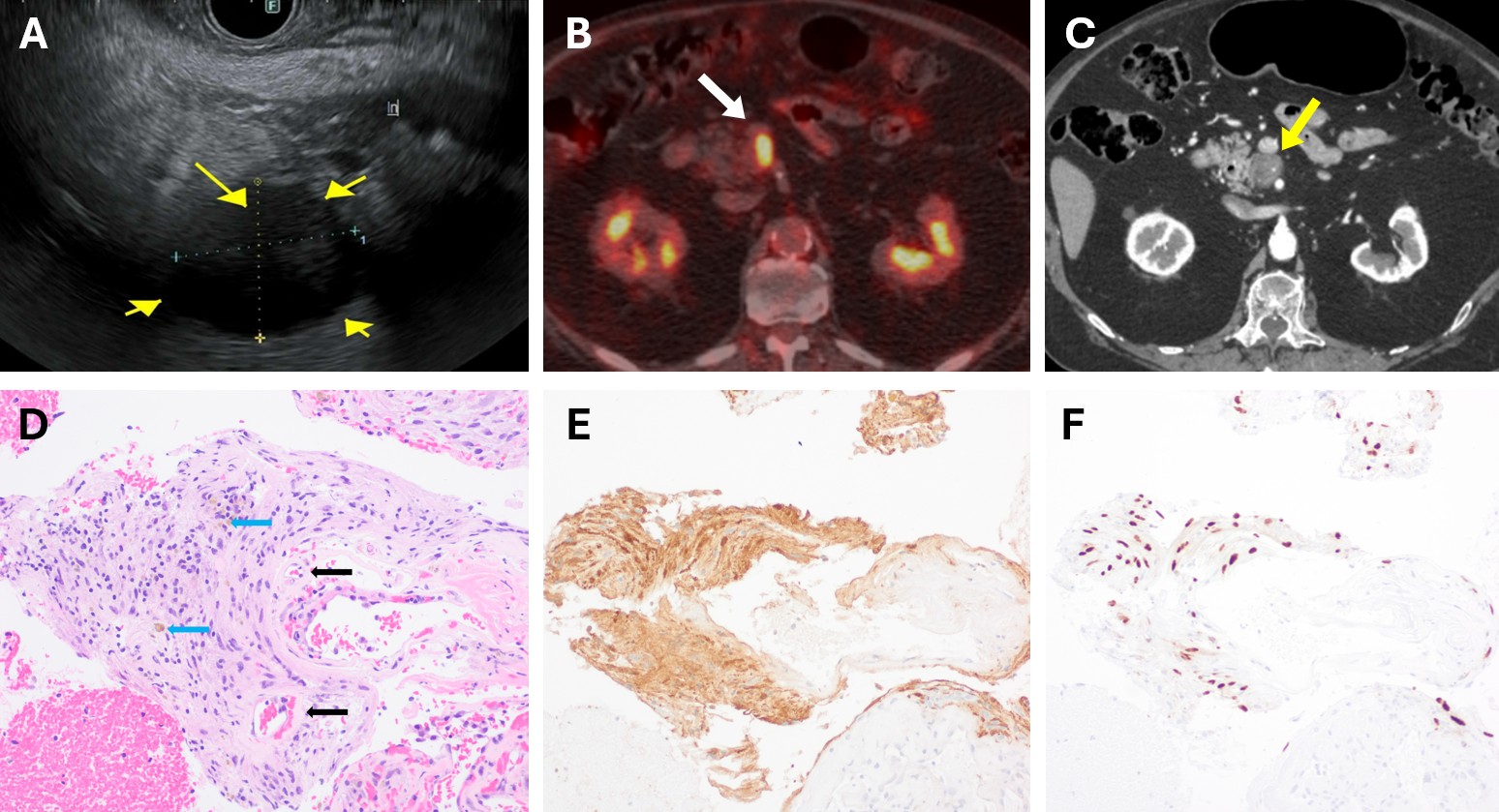
Methods: An 80-year-old man underwent an abdominal CT scan for bilateral lower limb edema, which revealed an enlarged solid lesion adjacent to the uncinate process. A PET/CT scan showed a 2.3×1.7 cm solid lesion medial to the uncinate process, suspicious for malignancy due to high metabolic activity. Serum CA 19-9 and CEA levels were undetectable. To further characterize the lesion, the patient underwent an EUS, which showed a 2.4×2.0 cm well-defined peripancreatic hypoechoic lesion with a cystic component. Fine needle biopsy was performed, and histology showed positive staining for S-100 and SOX10, and negative staining for CD117, confirming the diagnosis of pancreatic schwannoma. The patient met with the surgery team, and the decision was conservative management given his age and comorbidities. Follow-up CT scans at 3 and 12 months showed no morphological changes. Discussion: Pancreatic schwannomas are rare tumors, representing less than 1% of all schwannomas, and have a low risk of malignant transformation. Despite their benign nature, factors that may suggest potential malignancy include increasing tumor size and high mitotic activity (e.g., Ki-67). CT and MRI cannot reliably distinguish benign from malignant lesions, whereas EUS with fine needle biopsy allows a more accurate diagnosis. Pancreatic schwannomas should be considered in the differential diagnosis of cystic pancreatic lesions. Although surgery remains the definitive treatment, conservative management with regular surveillance is a feasible and appropriate option in selected patients.
Figure: A) EUS showing a peripancreatic lymph node. B) PET/CT scan revealing a lymph node with metabolic activity. C) Follow-up CT scan demonstrating no radiological changes. D) H&E, 20×: benign spindle cell proliferation with hemosiderin pigment (blue arrows) and hyalinized vessels (black arrows). E) S100 protein, 20×: spindle cells show positive staining in both the nucleus and cytoplasm, and F) SOX10, 20×: spindle cells show nuclear positivity; both findings confirm Schwann cell origin.
Disclosures: David Guevara-Lazo indicated no relevant financial relationships. Jonathan McHugh indicated no relevant financial relationships. Jorge Machicado indicated no relevant financial relationships.
David Guevara-Lazo, MD, Jonathan B.. McHugh, MD, Jorge D.. Machicado, MD, MPH. P2353 - Pancreatic Schwannoma: An Unexpected Cause of Peripancreatic Mass, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")