Tia D. Andrade, MD, Houda Abdelrahman, MD Beth Israel Deaconess Medical Center, Boston, MA Introduction: Lipoprotein X (LpX) is a rare dyslipidemia caused by cholestatic biliary disease when biliary contents reflux into the serum. As such, the definitive treatment is liver transplantation that replaces the diseased biliary tree. Because LpX lacks apoplipoprotein B (apoB), hyperlipidemia treatments that focus on increasing LDL-receptor density and uptake are not effective. While the atherogenicity of LpX is debated, LpX accumulation leads to kidney disease. Other complications are being explored. This case discusses the disease course of LpX and plasmapheresis management as a temporizing treatment in a patient ineligible for transplantation.
Case Description/
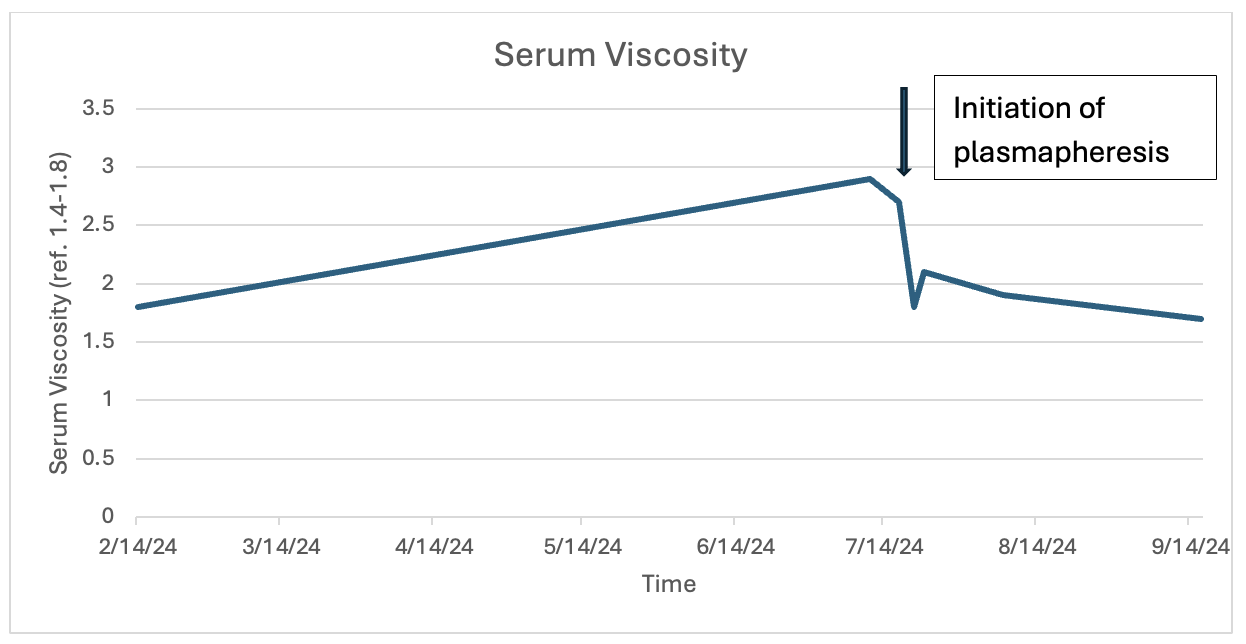
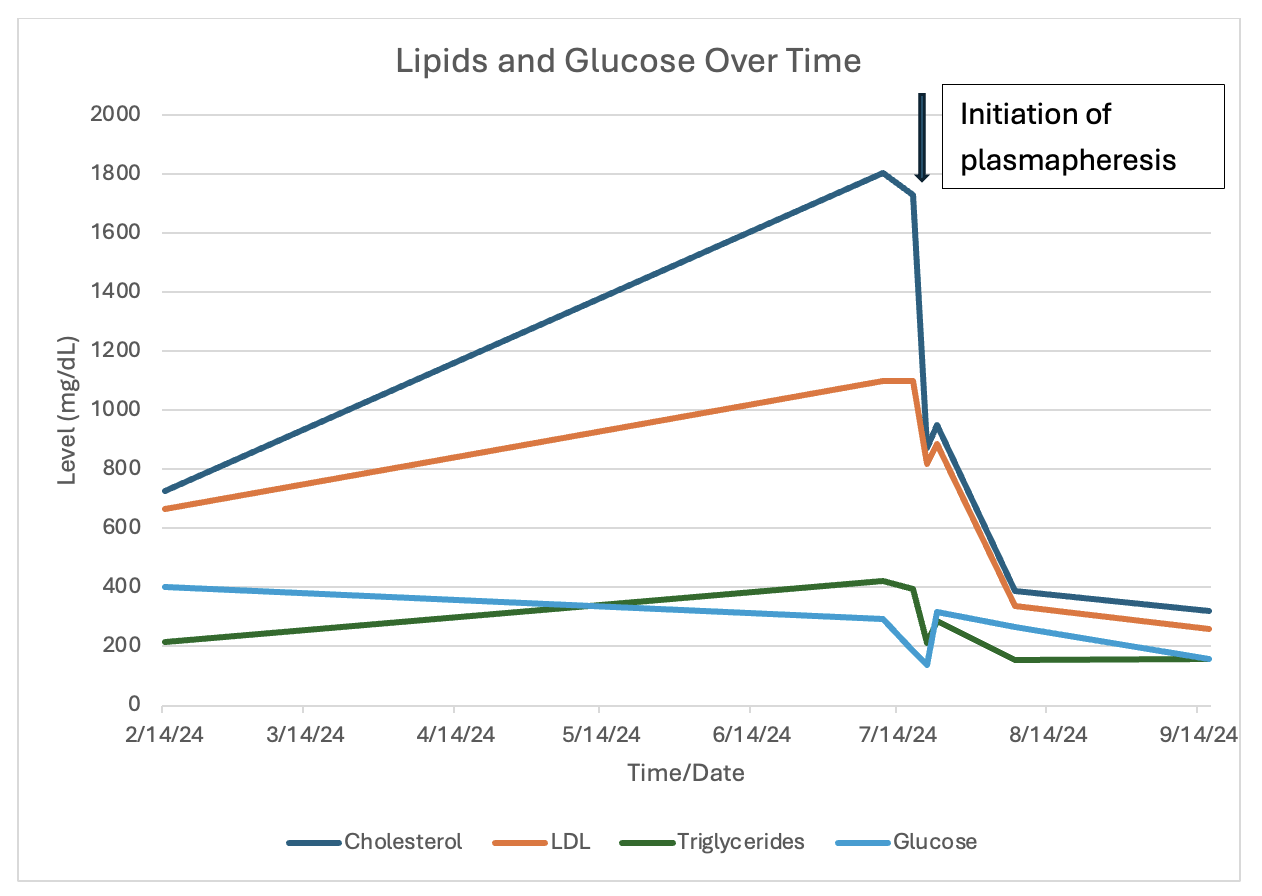
Methods: A 28-year-old female with history of gallstone pancreatitis treated with ERCP and laparoscopic cholecystectomy developed progressive liver failure 6 months after her initial surgery and was admitted for liver transplantation evaluation. She had developed xanthomas and increasing insulin requirements with persistent hyperglycemia. NMR spectroscopy and agarose gel electrophoresis confirmed the diagnosis of LpX causing lipotoxicity and peripheral insulin resistance. While MRCP showed biliary dilation and strictures, biopsy confirmed secondary sclerosing cholangitis. Discussion: The patient was denied liver transplantation due to insurance coverage. Lipid lowering medications would be ineffective at reducing lipid levels. After reporting remote history of nose bleeds with concern for hyperviscosity syndrome, the patient was initiated on plasmapheresis with significant improvement in lipid levels, hyperglycemia, and serum viscosity (Figure 1 & 2). She was discharged with plans to list for liver transplantation at another institution.
Insulin resistance and hyperviscosity syndrome are additional complications of LpX. Plasmapheresis is an effective temporizing treatment for lowering glucose and lipid levels, thus reducing serum viscosity. However, liver transplantation is the definitive treatment.
Figure: Change in lipid levels and glucose over time with initiation of plasmapheresis.
Figure: Change in serum viscosity over time with initiation of plasmapheresis.
Disclosures: Tia Andrade indicated no relevant financial relationships. Houda Abdelrahman indicated no relevant financial relationships.
Tia D. Andrade, MD, Houda Abdelrahman, MD. P2349 - Management of Lipoprotein X in a Patient With Secondary Sclerosing Cholangitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.