Monday Poster Session
Category: Colon
Ananya Venkatesh, MD
Thomas Jefferson University Hospital
Philadelphia, PA
A 70-year-old male presented with three weeks of abdominal pain, tenesmus, and hematochezia. Physical examination revealed periumbilical tenderness with guarding. Laboratory studies demonstrated an ESR 21 mm/hr, CRP 62.9 mg/L, and fecal calprotectin 503 µg/g. Complete blood count, rheumatologic panel, and infectious stool studies were unremarkable. Contrast-enhanced CT showed bowel wall thickening from the distal descending colon to the rectum with pericolonic fat stranding. He was initially managed with antibiotics and bowel rest.
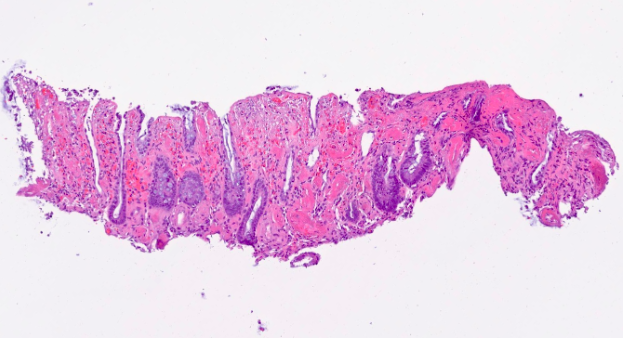
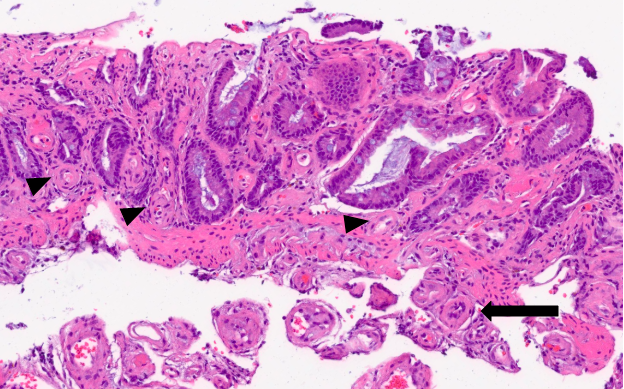
Subsequent CT angiography demonstrated patent mesenteric arteries but notable ectasia and tortuosity of several inferior mesenteric artery branches. Colonoscopy showed mucosal edema, erythema, and ulcerations from the rectum to the descending colon. Intravenous methylprednisolone was initiated for a presumed diagnosis of IBD. However, histopathology revealed colonic mucosa with severe ischemic injury and necrosis, with features suggestive of IMHMV (Figure 1). Due to clinical deterioration despite maximal medical therapy, the patient underwent sigmoid colectomy. The resected specimen demonstrated cardinal features of IMHMV such as marked thickening of the mesenteric veins with associated luminal narrowing. (Figure 2).