Sepideh Mehravar, MD, Aida Pirvaram, MD, Ali Rezaie, MD, MSc Cedars-Sinai Medical Center, Los Angeles, CA Introduction: Partial small bowel obstruction (pSBO) often occurs due to post-surgical adhesions. Surgical lysis of adhesions is often non-curative and carries risks, so conservative in-patient care with bowel rest is preferred. We present a case of recurrent pSBO managed as an outpatient with a palatable elemental diet (PED), highlighting its non-invasive potential.
Case Description/
Methods: A 46-year-old woman with a complex gastrointestinal surgical history presented for follow-up due to worsening gastrointestinal symptoms. Her medical history was significant for colonic inertia and prior laxative dependence, for which she underwent a total colectomy 10 years ago complicated by an anastomotic leak that necessitated a temporary diverting ileostomy which was later reversed. Since then, her clinical course has been complicated by multiple episodes of pSBO, averaging 1–2 episodes per year. Obstructive episodes were presumed to be secondary to postoperative adhesions and required hospitalizations with nasogastric tube decompression, complete bowel rest and temporary parenteral nutrition. Given her prior postoperative complications, she has been understandably hesitant to undergo surgical lysis of adhesions.
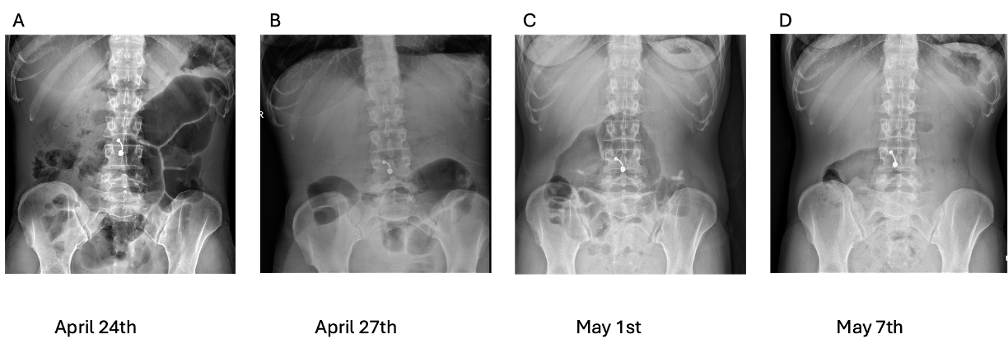
Episodes of pSBO would occur despite multiple gut-directed treatments including lubiprostone, linaclotide, plecanatide, pyridostigmine, and rifaximin daily. She had a pSBO recurrence in 2024. While maintain the existing medications, she was transitioned to a two-week course of eucaloric exclusive oral PED (mBIOTA elemental). Serial abdominal radiographs revealed decreased small bowel dilation and resolution of air-fluid levels correlating with clinical improvement. A follow-up abdominal X-ray one month later continued to show radiographic improvement. Her weight remained stable during this period (Figure 1, panels A–D).
Approximately one year later in 2025, she re-presented with abdominal discomfort, distention, and nausea without obstipation or vomiting compatible with recurrence of pSBO. Again she was to a two-week course of eucaloric exclusive oral PED which led to radiologic and symptomatic resolution of pSBO (Figure 2). Discussion: This case highlights that outpatient management of pSBO without alarm features is feasible with the use of an exclusive oral PED. Elemental diets provide complete nutrition with high absorptive efficiency in the proximal small bowel. Being fiber- and residue-free, they present an intriguing option for the conservative management of partial bowel obstruction.
Figure: Figure 1) Serial abdominal radiographs demonstrating the progression and resolution of partial small bowel obstruction in response to outpatient exclusive elemental diet consumption in 2024.
Figure: Figure 2) Serial abdominal radiographs demonstrating the progression and resolution of partial small bowel obstruction in response to outpatient elemental diet consumption in 2025.
Disclosures: Sepideh Mehravar indicated no relevant financial relationships. Aida Pirvaram indicated no relevant financial relationships. Ali Rezaie: Ardelyx, Blueprint Medicine and Salix Pharmaceuticals – Consultant. Gemelli Biotech, and Good LFE – Equity stake.
Sepideh Mehravar, MD, Aida Pirvaram, MD, Ali Rezaie, MD, MSc. P2720 - Outpatient Management of Partial Small Bowel Obstruction Using an Oral Palatable Elemental Diet, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.