P2800 - Impact of Radiofrequency Ablation Energy Settings on Risk of Recurrence After Complete Remission of Intestinal Metaplasia in Barrett’s Esophagus
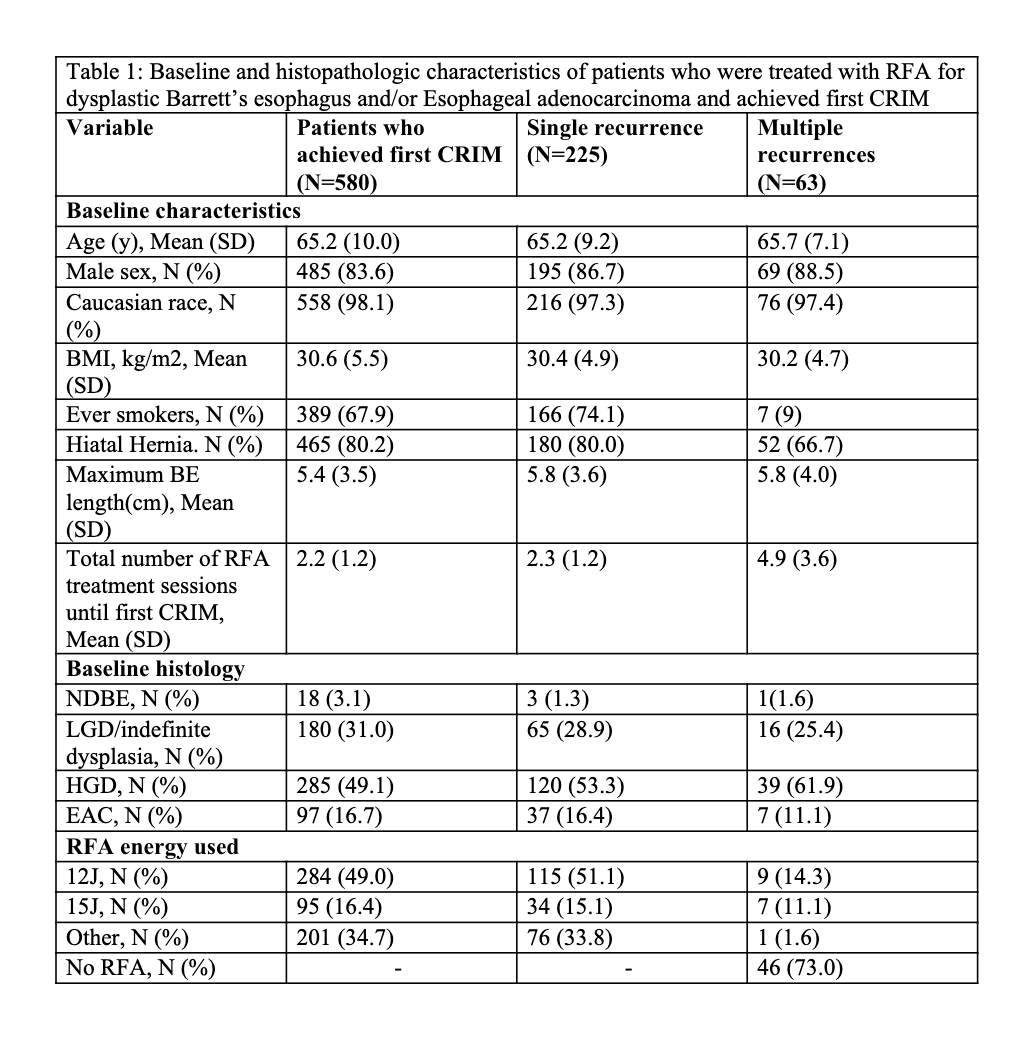
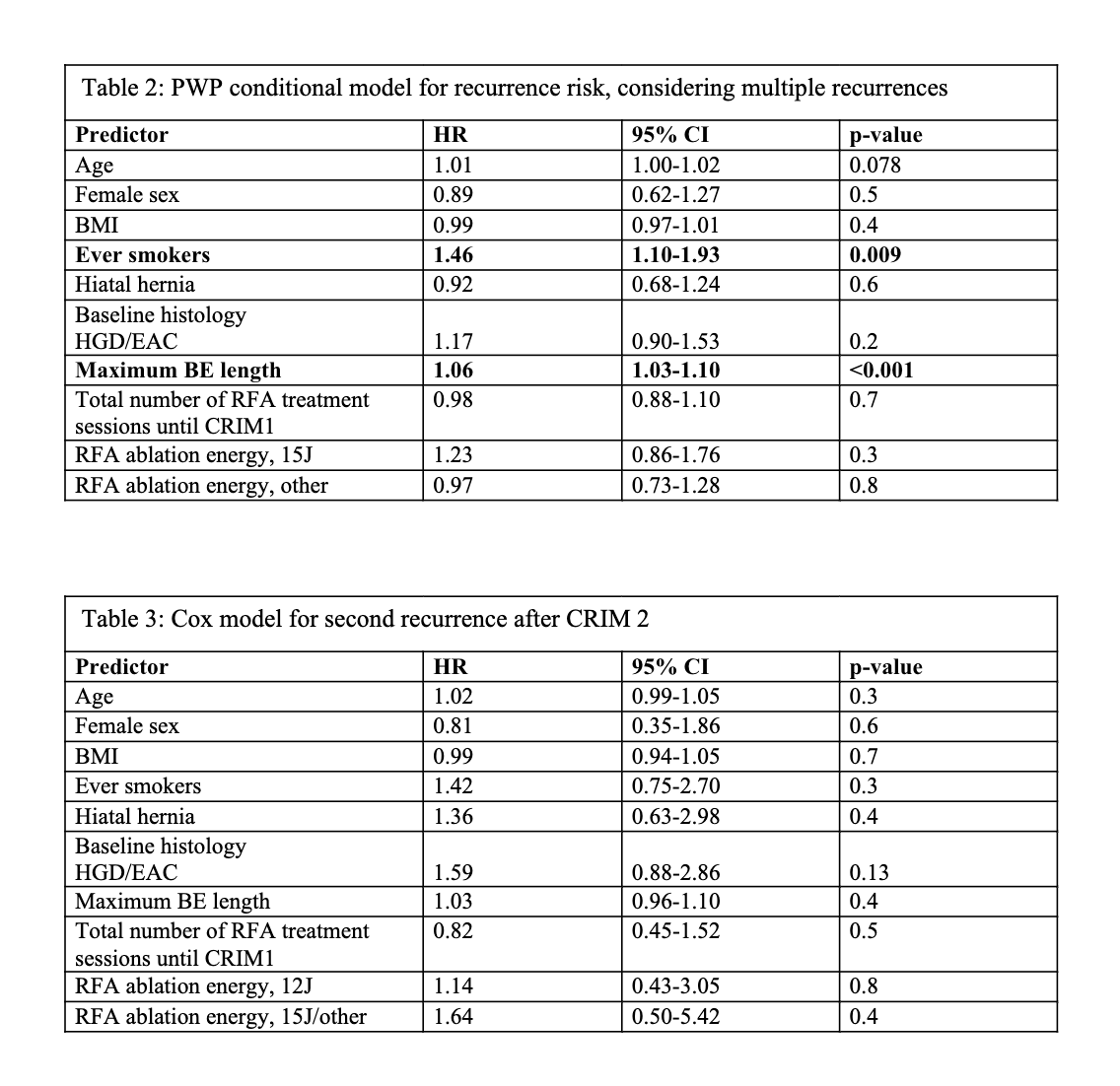
Vanya Rai, MBBS1, Anjul Verma, MD2, Paras Singh Chandi, MBBS3, Sandra Algarin-Perneth, MD1, Melissa Passe, MSN1, Ramona Lansing, RN1, Caryn Anderson, 1, Cadman Leggett, MD1, Swathi Eluri, MD, MSCR4, Prasad Iyer, MD, MS5, Don C. Codipilly, MD1 1Mayo Clinic, Rochester, MN; 2Texas Tech University Health Sciences Center, Odessa, TX; 3Cook County Health, Chicago, IL; 4Mayo Clinic, Jacksonville, FL; 5Mayo Clinic, Phoenix, AZ Introduction: The impact of focal radiofrequency ablation (RFA) energy settings on recurrence risk after complete remission of intestinal metaplasia (CRIM) is unclear following endoscopic eradication therapy (EET) for Barrett’s esophagus (BE). Methods: We retrospectively analyzed 580 patients who achieved CRIM following RFA for dysplastic BE or intramucosal adenocarcinoma (IMCa) at a high-volume center between 2003-2024. CRIM was defined as the first histologic confirmation of absence of IM following EET. Recurrence was defined as any detection of IM, dysplasia or IMCa on surveillance biopsies after CRIM. Patients were stratified based on the energy used: 12J (12Jx2 per treatment site covering entire BE segment, coagulum cleaned, then repeat 12Jx2; n=284), 15Jx3 per treatment site covering entire BE segment; n=95), or mixed/other (n=201). Outcomes assessed included incidence of first and second recurrence and recurrence histology. A PWP conditional Cox model evaluated predictors of multiple recurrences. A secondary Cox model assessed predictors of second recurrence after CRIM2. Results: 225 (38.8%) CRIM patients developed recurrence during a median follow up of 3.7 years (IQR: 1.3-6.7). Table 1 summarizes baseline characteristics. The recurrence rates per 100 person-years were: 12J (12.8), 15J (15.6), and other (13.5). In the PWP model, increasing BE segment length (HR 1.06; 95% CI 1.03–1.10; p< 0.001) and smoking history (HR 1.46; 95% CI 1.10–1.93; p=0.009) were significantly associated with recurrence, but not variability in RFA energy delivery (Table 2). Of those with recurrence, 52 underwent repeat RFA and achieved CRIM2. 19 patients among these developed a second recurrence. Second recurrence rates per 100 person-years were: no RFA (16.5), 12J (13.9), 15J/other (21.2). In the Cox model for second recurrence, energy delivery was not associated with recurrence risk. However, a dysplastic first recurrence was associated with a higher likelihood of dysplastic second recurrence (16.7% vs. 5.4%, p< 0.01) (Table 3). Discussion: While RFA energy was not associated with recurrence, patients treated with 15J had numerically higher recurrence rates. Smoking and longer BE segment length remained significant recurrence predictors. Importantly, dysplastic first recurrence substantially increased the risk of a dysplastic second recurrence, emphasizing the need for closer surveillance in this subgroup. Future prospective evaluation of energy dosing and recurrence risk is warranted.
Figure: Baseline and histopathologic characteristics of patients who were treated with RFA for dysplastic Barrett’s esophagus and/or Esophageal adenocarcinoma and achieved first CRIM.
Figure: PWP conditional model for recurrence risk, considering multiple recurrences and Cox model for second recurrence after CRIM 2.
Disclosures: Vanya Rai indicated no relevant financial relationships. Anjul Verma indicated no relevant financial relationships. Paras Singh Chandi indicated no relevant financial relationships. Sandra Algarin-Perneth indicated no relevant financial relationships. Melissa Passe indicated no relevant financial relationships. Ramona Lansing indicated no relevant financial relationships. Caryn Anderson indicated no relevant financial relationships. Cadman Leggett indicated no relevant financial relationships. Swathi Eluri indicated no relevant financial relationships. Prasad Iyer: CDx medical – Consultant, Grant/Research Support. Exact – Grant/Research Support. Exact Sciences – Consultant, Grant/Research Support. Medtronic – Consultant. Pentax Medical – Consultant, Grant/Research Support. Don Codipilly indicated no relevant financial relationships.
Vanya Rai, MBBS1, Anjul Verma, MD2, Paras Singh Chandi, MBBS3, Sandra Algarin-Perneth, MD1, Melissa Passe, MSN1, Ramona Lansing, RN1, Caryn Anderson, 1, Cadman Leggett, MD1, Swathi Eluri, MD, MSCR4, Prasad Iyer, MD, MS5, Don C. Codipilly, MD1. P2800 - Impact of Radiofrequency Ablation Energy Settings on Risk of Recurrence After Complete Remission of Intestinal Metaplasia in Barrett’s Esophagus, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")