Central Michigan University College of Medicine Saint Joseph, MI
Sarah Ecenbarger, BS, BA1, Thomas Birris, MD2 1Central Michigan University College of Medicine, Saint Joseph, MI; 2Corewell Health Lakeland, Saint Joseph, MI Introduction: Gastrocolic fistula, an abnormal connection between the stomach and colon, is a very rare and severe complication with unknown incidence which most commonly occurs due to gastric or colonic adenocarcinoma. However, we report a case of a large gastrocolic fistula secondary to benign gastric ulcer in an asymptomatic patient, which was easily traversed during endoscopy.
Case Description/
Methods: A 56-year-old female with a past medical history of chronic back pain on non-steroidal anti-inflammatory drugs (NSAIDs) and schizoaffective disorder (bipolar-type), was referred to the emergency department regarding severe anemia. Anemia was discovered on a complete blood count (CBC) obtained as part of lamotrigine medication monitoring. The patient was reportedly asymptomatic and denied hematemesis, melena, and hematochezia. CBC revealed a hemoglobin of 5.7 g/dL with microcytosis. Iron studies further uncovered an iron level of 11 mcg/dL and a ferritin of < 8 ng/mL. Bidirectional endoscopy was pursued to evaluate for a source of iron deficiency anemia. Esophagogastroduodenoscopy (EGD) revealed liquid stool in the stomach, and a large gastric ulcer complicated by fistula to the colon, through which the gastroscope could easily pass. Colonoscopy followed EGD, which confirmed patency of the fistula bidirectionally. Multiple forceps biopsies were performed from either side of the fistula, as well as from the gastric body and antrum, and were found to be negative for both Helicobacter pylori and malignancy. An abdominal computed tomography scan with contrast confirmed fistulation with no evidence of extraluminal contrast or perforation of bowel contents into the peritoneum. Surgical repair was completed by open transverse colectomy and takedown of the fistula. The pathology of the transverse colectomy specimen with attached gastrocolic fistula confirmed its benign nature. Discussion: Gastrocolic fistula is extraordinary, with the most common etiology being malignancy; therefore, our case is uncommon. This is the first reported case of gastrocolic fistula secondary to NSAID overdose in a patient with schizoaffective disorder presenting solely as iron deficiency anemia. Clinicians must be aware of this possibility even when a patient is otherwise asymptomatic.
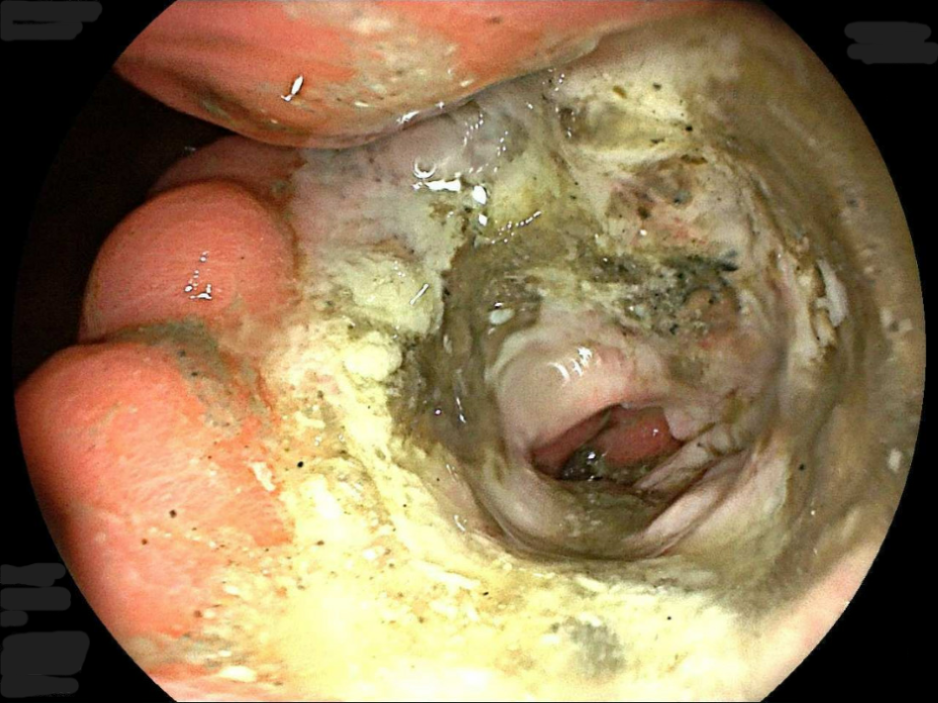
Figure: Gastrocolic fistula as seen on endoscopy
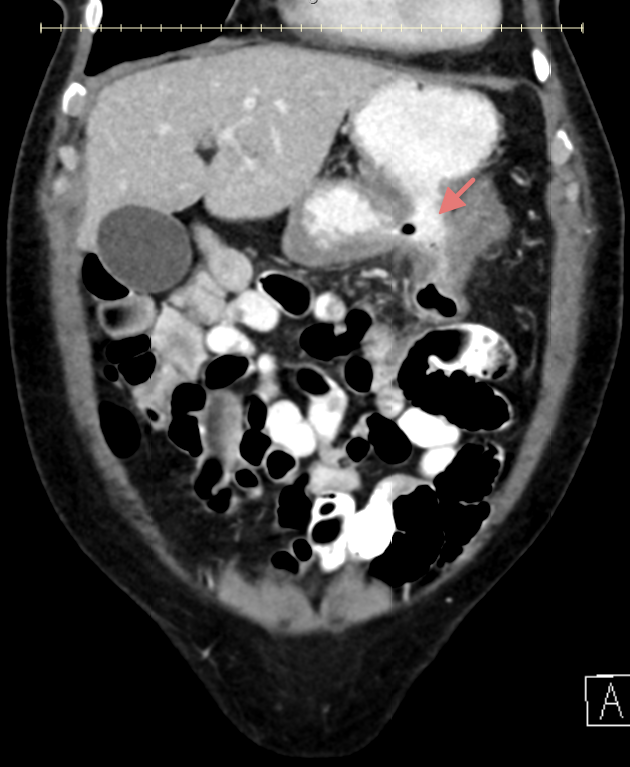
Figure: Gastrocolic fistula on CT scan
Disclosures: Sarah Ecenbarger indicated no relevant financial relationships. Thomas Birris: BMS – Speakers Bureau.
Sarah Ecenbarger, BS, BA1, Thomas Birris, MD2. P3041 - Stool in the Stomach? A Rare Case of Gastrocolic Fistula Secondary to Benign Peptic Ulcer -- Easily Traversable on Endoscopy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")