Staten Island University Hospital, Northwell Health Staten Island, NY
Joelle Sleiman, MD, Ahmed Elfiky, MD, Hassan Al Moussawi, MD, Jean Chalhoub, MD, Youssef El Douaihy, MD, Sherif Andrawes, MD Staten Island University Hospital, Northwell Health, Staten Island, NY Introduction: Primary signet ring cell carcinoma (SRCC) of the rectum is an uncommon and aggressive histologic subtype of colorectal cancer, accounting for 0.6–2.7% of all colorectal cancers. Unlike the more frequently encountered gastric SRCC, primary rectal SRCC is characterized by its rarity, advanced stage at diagnosis, and poor prognosis. This report aims to contribute to the limited body of literature on primary rectal SRCC and to highlight the importance of thorough diagnostic evaluation, as early detection is challenging due to the nonspecific or subtle presentation of endoscopic features.
Case Description/
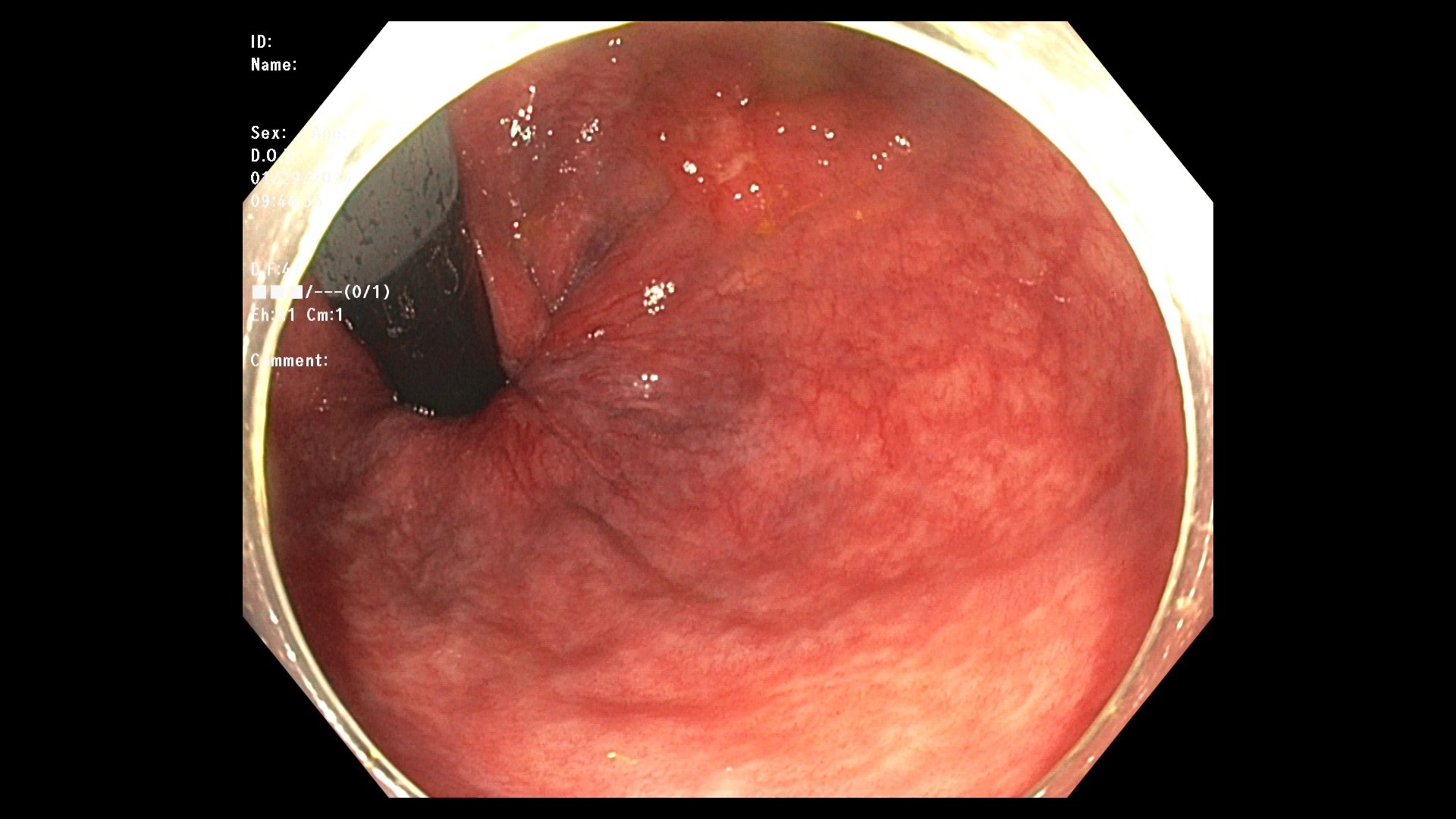
Methods: A 65-year-old male with a medical history of hypertension and gastroesophageal reflux disease presented for routine colorectal cancer screening. He reported no gastrointestinal symptoms, and there was no family history of gastrointestinal malignancies. Patient underwent colonoscopy, which revealed a 2.5 cm flat lesion with central depression in the rectum, just above the dentate line. The lesion was classified as Paris 0-IIa+0-III, and biopsies were obtained from both the center and periphery (Fig.1-2). Histopathological analysis revealed a tubulovillous adenoma in the peripheral biopsy and a poorly differentiated carcinoma with signet ring cell features in the central biopsy. Immunohistochemical staining showed positivity for CDX2, CK20, and SATB2, and negativity for CK7, consistent with colorectal origin. Mismatch repair protein expression was intact, indicating a low probability of microsatellite instability-high (MSI-H) and suggesting a low likelihood of Lynch syndrome. An esophagogastroduodenoscopy (EGD) was performed to rule out a gastric primary. The EGD revealed fundic gland polyps and erosive gastritis, but no evidence of malignancy. Discussion: In summary, this case highlights the clinical and pathological features of primary rectal SRCC without gastric involvement. The lesion's flat morphology with a central depression emphasizes the need for careful endoscopic evaluation, as such features may be subtle and easily overlooked. Given the aggressive nature and poor outcomes associated with rectal SRCC, early recognition and comprehensive management are critical.
Figure: Conventional white-light endoscopy demonstrates a flat rectal lesion with central depression.
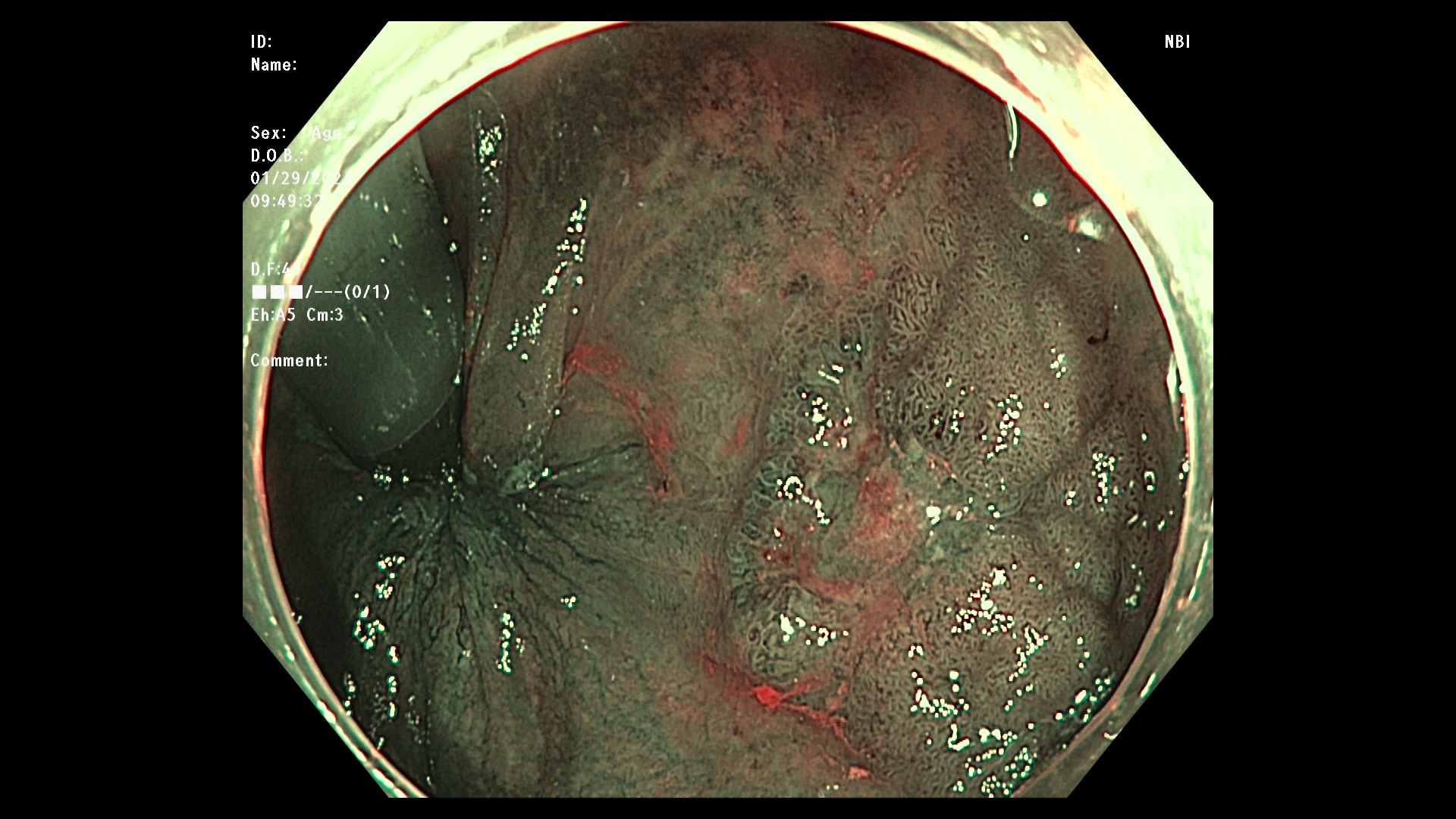
Figure: Narrow-band imaging reveals an irregular surface pattern and disrupted microvascular architecture, suggestive of neoplasia.
Disclosures: Joelle Sleiman indicated no relevant financial relationships. Ahmed Elfiky indicated no relevant financial relationships. Hassan Al Moussawi indicated no relevant financial relationships. Jean Chalhoub indicated no relevant financial relationships. Youssef El Douaihy indicated no relevant financial relationships. Sherif Andrawes indicated no relevant financial relationships.
Joelle Sleiman, MD, Ahmed Elfiky, MD, Hassan Al Moussawi, MD, Jean Chalhoub, MD, Youssef El Douaihy, MD, Sherif Andrawes, MD. P3035 - Isolated Rectal Signet Ring Cell Carcinoma During Routine Screening Colonoscopy: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.