NewYork-Presbyterian / Weill Cornell Medical Center New York, NY
Jade Wang, MD1, Lillian F. Zhang, MD, PhD1, Michelle Lee, MD1, Daniel Paik, MD, PhD1, Anthony J. Choi, MD1, Carolyn Newberry, MD1, Kartik Sampath, MD2, Evan Grossman, MD1 1NewYork-Presbyterian / Weill Cornell Medical Center, New York, NY; 2Weill Cornell Medicine, New York, NY Introduction: Variceal bleeding is a well-known cause of upper gastrointestinal (GI) bleeding in patients with cirrhosis. Varices most commonly arise in the gastro-esophageal region. Ectopic varices arise in other locations and are rarer but equally life-threatening causes of bleeding. We present a case of large-volume duodenal variceal bleed.
Case Description/
Methods: An 81-year-old woman with prior heavy alcohol use, dementia, and suspected cirrhosis presented for large-volume hematemesis and melena. She was tachycardic, with hemoglobin of 7.2 (from baseline 10.5) and elevated lactate. She was transfused with red blood cells and started on ceftriaxone, intravenous pantoprazole, and octreotide.
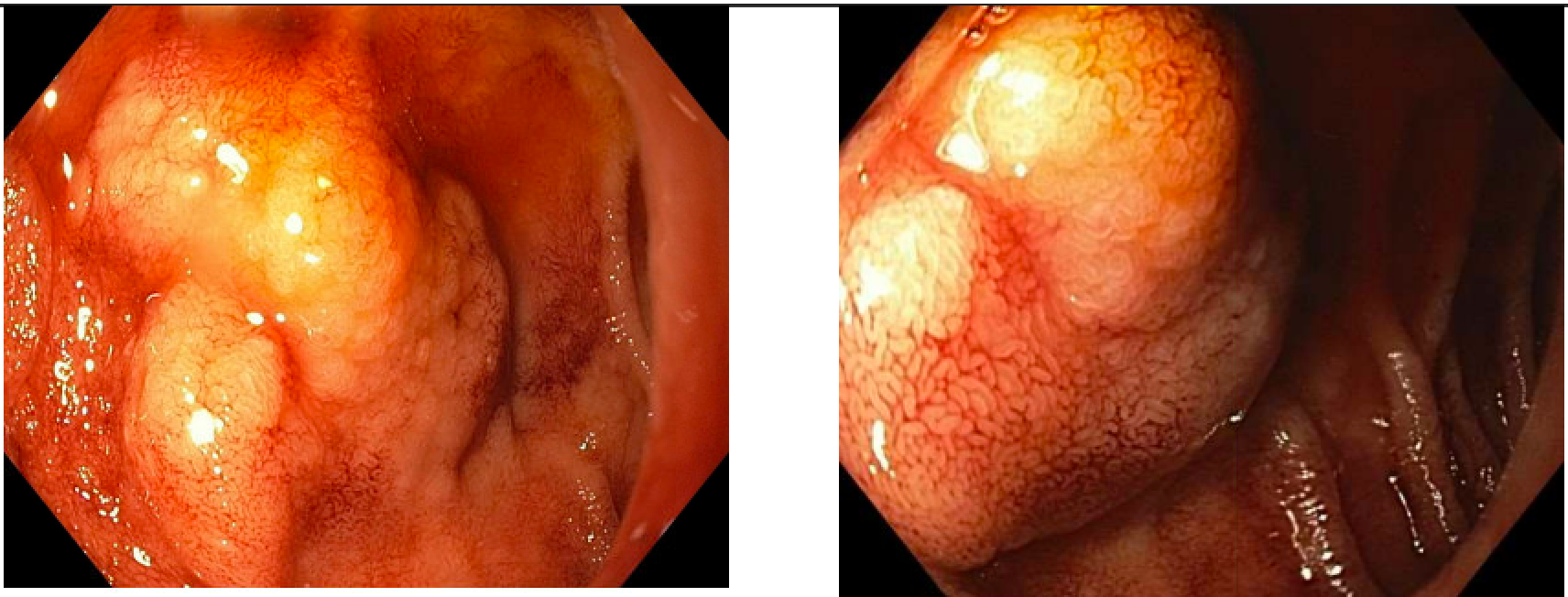
Computed tomography angiogram of the abdomen and pelvis showed cirrhotic liver morphology and paraduodenal varices. Esophagogastroduodenoscopy (EGD) showed blood and mucosal thickening in the first and second portions of the duodenum which flattened with time and insufflation (Figure 1). No active source of bleeding was seen. However, suspicion was high for duodenal varices as the source.
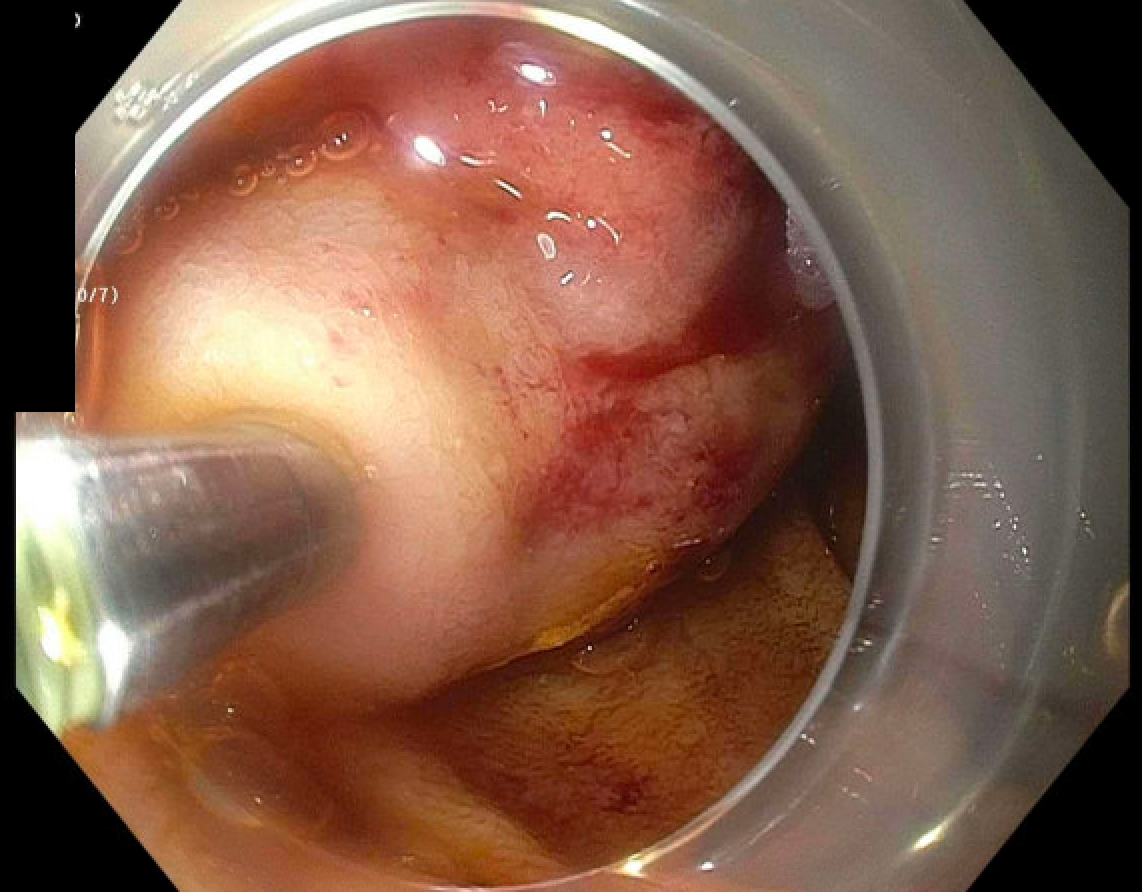
Treatment options including sclerosant injection therapy and transjugular intrahepatic portosystemic shunt (TIPS) were discussed with the patient’s healthcare proxy (HCP). Due to the patient’s advanced dementia and high Model for End-Stage Liver Disease score, she was not an appropriate TIPS candidate; it was agreed to proceed with injection. Repeat EGD with endoscopic ultrasound found large, actively bleeding Grade III varices in the duodenal sweep. The area was injected with cyanoacrylate (Figure 2). The procedure was tolerated well without further overt bleeding.
Following the procedure, per the wishes of the patient’s HCP, the patient was transitioned to home hospice. Discussion: Ectopic variceal bleeding accounts for about 5% of variceal bleeds. 25-33% of ectopic variceal bleeds are duodenal, and are most commonly found in the first and second portions of the duodenum. These present a diagnostic challenge given their rarity and should always be on the differential in cases of upper GI bleed. Management options for duodenal varices include banding, sclerosant injection therapy, embolization, and TIPS. TIPS is very effective at managing variceal bleeding by reducing portal hypertension. However, the risks of liver failure with encephalopathy and volume overload must be carefully weighed, and, as in this case, the patient’s medical comorbidities and preferences must be considered when choosing the most appropriate therapy.
Figure: Figure 1: Initial esophagogastroduodenoscopy (EGD) showed blood and mucosal thickening in the first and second portions of the duodenum which flattened with time and insufflation. No active source of bleeding was identified.
Figure: Figure 2: Injection of the duodenal varix with cyanoacrylate on repeat EGD.
Disclosures: Jade Wang indicated no relevant financial relationships. Lillian Zhang indicated no relevant financial relationships. Michelle Lee indicated no relevant financial relationships. Daniel Paik indicated no relevant financial relationships. Anthony Choi indicated no relevant financial relationships. Carolyn Newberry: Eli Lilly & Co – Consultant. Kartik Sampath: CONMED – Consultant. Evan Grossman indicated no relevant financial relationships.
Jade Wang, MD1, Lillian F. Zhang, MD, PhD1, Michelle Lee, MD1, Daniel Paik, MD, PhD1, Anthony J. Choi, MD1, Carolyn Newberry, MD1, Kartik Sampath, MD2, Evan Grossman, MD1. P3130 - A Case of Large-Volume Duodenal Variceal Bleed in a Patient With Suspected Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.