P3421 - Trends in Mortality Related to Gastrointestinal Cancers and Sepsis Among Older Adults in the United States Between 1999 and 2020: A Retrospective Analysis
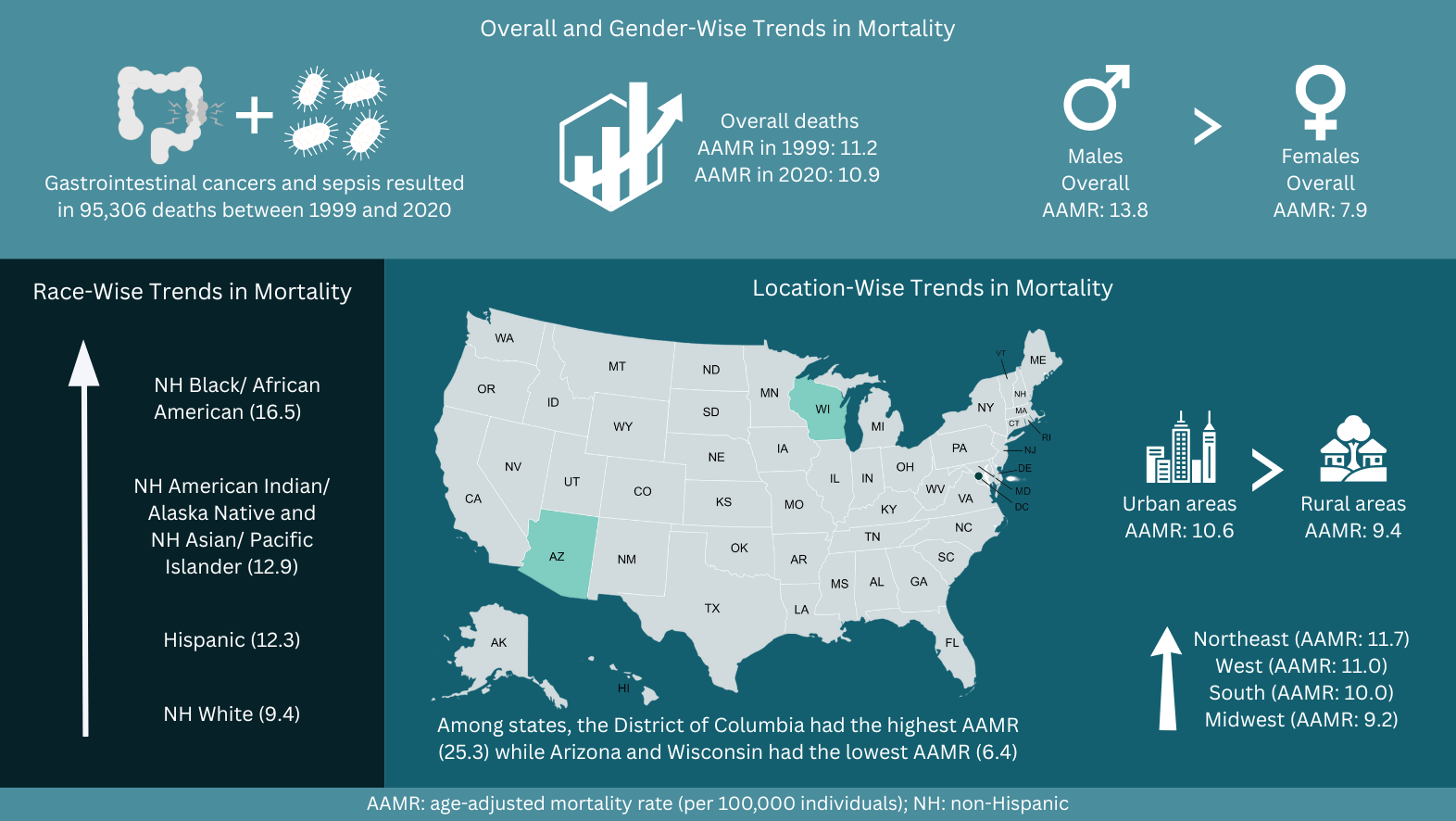
Abdul Ahad, MBBS1, Mustafa Shah, MD2, Kumail Mustafa Ali, MBBS3, Muhammad Haleem Nasar, MBBS4, Abdul Haseeb, MBBS5, Irfan Ullah, MBBS6 1Kabir Medical College, Peshawar, North-West Frontier, Pakistan; 2Geisinger Health System, Danville, PA; 3Jinnah Sindh Medical University, Karachi, Sindh, Pakistan; 4Northwest School of Medicine, Peshawar, North-West Frontier, Pakistan; 5Northwest General Hospital and Research Centre, Peshawar, North-West Frontier, Pakistan; 6Khyber Teaching Hospital, Peshawar, North-West Frontier, Pakistan Introduction: Sepsis is a major cause of illness and death in patients with gastrointestinal (GI) cancers due to immunosuppression, hospitalizations, and treatment-related risks. GI cancers now make up over 25% of global cancer cases. However, data on deaths from both sepsis and GI cancer are limited. This study aims to examine GI cancer and sepsis-related mortality trends in older adults in the United States (US). Methods: Data were sourced from the Centers for Disease Control and Prevention’s Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) multiple cause-of-death database from 1999-2020 for concomitant GI cancer and sepsis mortality in adults ≥65 years in the US. Age-adjusted mortality rates (AAMRs) per 100,000 persons, with 95% confidence intervals (CIs), were calculated and stratified by year, sex, race, region, and urbanization status. Average annual percent changes (AAPC) and Annual percent changes (APC) were computed using Joinpoint regression. Results: From 1999 to 2020, 95,306 deaths occurred due to GI cancer and sepsis. The Overall AAMR remained stable during the study period, ranging from 11.2 in 1999 to 10.9 in 2020 (AAPC: -0.06; 95% CI: -0.27 to 0.39). The overall AAMR steadily declined until 2013 (APC: -1.02; 95% CI: -2.24 to 1.33), followed by a steady incline until 2018 (APC: 2.97, 95% CI: -3.83 to 5.49) and then stabilizing in 2020 (APC: -0.76; 95% CI: -3.28 to 2.18). Males (13.8) had higher overall AAMRs than females (7.9). Non-Hispanic (NH) Blacks had the highest AAMR at 16.5, followed by NH American Indians/Alaska Natives and NH Asians/Pacific Islanders at 12.9, Hispanics at 12.3, and NH Whites at 9.4. Geographically, the Northeast (11.7) and urban areas (10.6) showed the highest AAMRs. Among states, the District of Columbia had the highest AAMR at 25.3, while Arizona and Wisconsin had the lowest at 6.4. Discussion: Although overall GI cancer and sepsis-related mortality among older adults remained stable from 1999 to 2020, sociodemographic disparities persisted, with males, NH Black individuals, Northeast residents, and urban populations bearing the highest burden. These findings underscore the importance of earlier sepsis recognition, enhanced infection control measures, refined oncology sepsis protocols, and improved access to cancer care for high-risk groups. Further research is needed to explore the drivers of these trends and assess interventions to lower GI cancer and sepsis-related deaths in elderly patients.
Figure: Figure 1. Gastrointestinal cancers and sepsis-related mortality trends among older adults in the United States, 1999 to 2020.
Disclosures: Abdul Ahad indicated no relevant financial relationships. Mustafa Shah indicated no relevant financial relationships. Kumail Mustafa Ali indicated no relevant financial relationships. Muhammad Haleem Nasar indicated no relevant financial relationships. Abdul Haseeb indicated no relevant financial relationships. Irfan Ullah indicated no relevant financial relationships.
Abdul Ahad, MBBS1, Mustafa Shah, MD2, Kumail Mustafa Ali, MBBS3, Muhammad Haleem Nasar, MBBS4, Abdul Haseeb, MBBS5, Irfan Ullah, MBBS6. P3421 - Trends in Mortality Related to Gastrointestinal Cancers and Sepsis Among Older Adults in the United States Between 1999 and 2020: A Retrospective Analysis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.