P3549 - Safety and Efficacy of Hybrid Endoscopic Submucosal Dissection-Endoscopic Mucosal Resection for Large Polyps at the Ileocecal Valve: A Retrospective Single Center Study
University of Minnesota Medical Center Minneapolis, MN
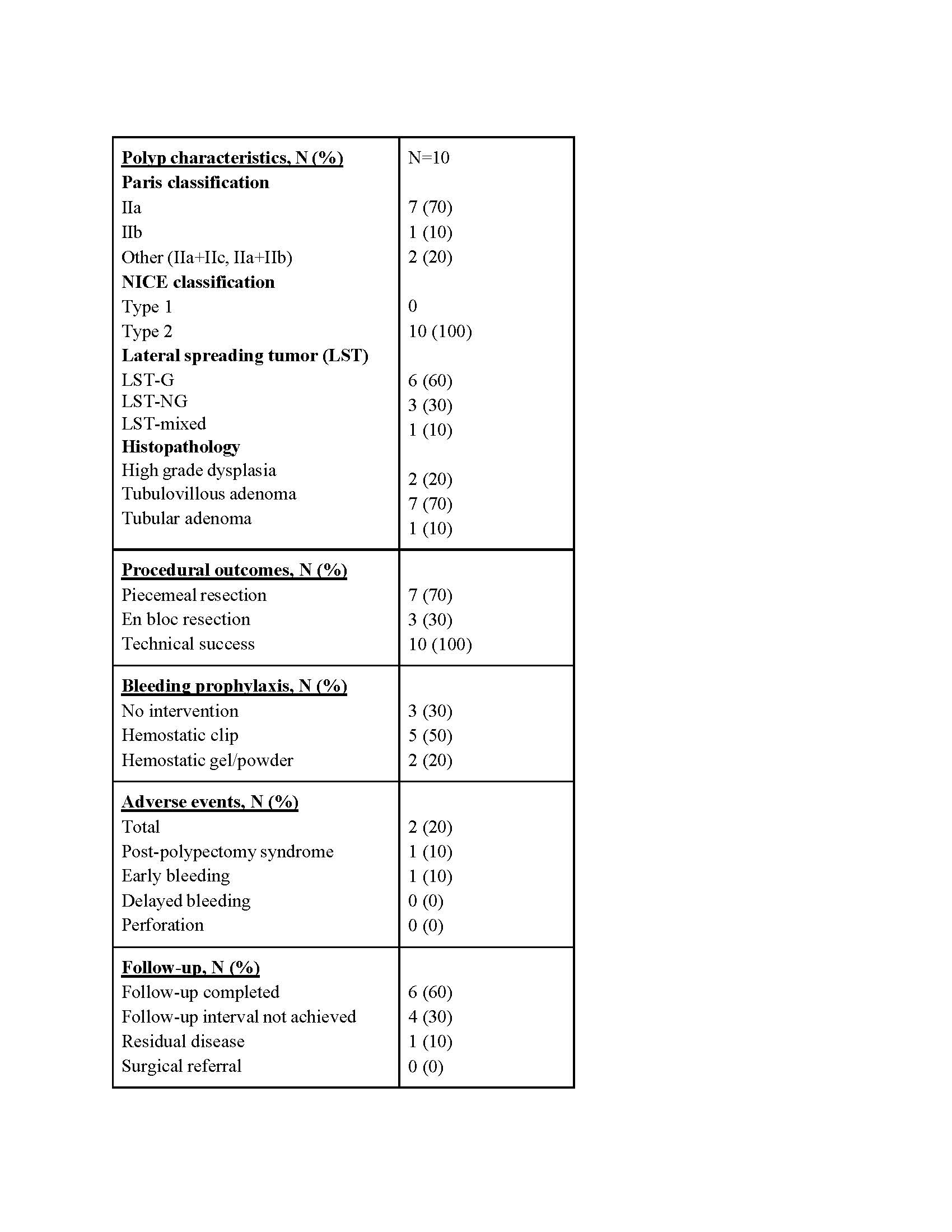
Taylor Bowler, DO1, Rahul Karna, MD1, Abubaker Abdalla, MD1, Nabeel Azeem, MD2 1University of Minnesota Medical Center, Minneapolis, MN; 2University of Minnesota, Minneapolis, MN Introduction: Endoscopic resection of polyps at the ileocecal valve (ICV) can be challenging due to anatomic complexity including polyp extension into the terminal ileum and polyp flatness. Hybrid endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) is a technique that allows for initial submucosal dissection of polyp margins prior to EMR, allowing for reduced recurrence rates while avoiding potential adverse events of ESD. In this study, we report a case series of 10 adult patients with ICV polyps who underwent successful endoscopic resection utilizing hybrid ESD-EMR and outline the safety and efficacy of the technique. Methods: We performed a retrospective review of patients who underwent endoscopic resection of ICV polyps at University of Minnesota Medical Center from 2022 to 2025. Patients who underwent hybrid ESD-EMR technique were included in our study. Data on polyp characteristics and histopathology, procedural outcomes, interventions used for bleeding prophylaxis, adverse event rates, recurrence rates and surgical referral were obtained. Descriptive statistics were used to analyze the data. Results: 10 patients with ICV polyps who underwent hybrid ESD-EMR were included. Study population consisted of 40% males with a mean age of 61.6 years. The median polyp size was 20 mm (10-50 mm). Additional polyp characteristics are outlined in Table 1. Technical success was 100%. 70% of lesions were resected in piecemeal fashion and 30% using en-bloc resection. Interventions for bleeding prophylaxis were variable: hemostatic clips for 50% of cases, hemostatic powder for 20%, and no intervention for the remaining 30% of cases. Final histopathology was high grade dysplasia in 20% of cases. Adverse events were noted in 20% of cases, consisting of one patient with post-polypectomy syndrome (ASGE grade I) and one patient with early bleeding (ASGE grade IIIa). One patient who underwent piecemeal resection had residual disease on six-month follow-up and underwent cold snare resection followed by hot avulsion. None of the patients required surgical referral after endoscopic resection. Discussion: Our case series demonstrates 100% technical success with a minimal risk of disease recurrence or adverse events. We conclude that hybrid ESD-EMR may be a safe and effective resection strategy for management of large polyps at the ICV. Challenges remain with prevention of delayed bleeding as prophylactic clip closure is often difficult and can potentially cause stenosis at the ICV.
Figure: Table 1: Summary of polyp characteristics and procedural outcomes
Disclosures: Taylor Bowler indicated no relevant financial relationships. Rahul Karna indicated no relevant financial relationships. Abubaker Abdalla indicated no relevant financial relationships. Nabeel Azeem: Boston Scientific – Consultant.
Taylor Bowler, DO1, Rahul Karna, MD1, Abubaker Abdalla, MD1, Nabeel Azeem, MD2. P3549 - Safety and Efficacy of Hybrid Endoscopic Submucosal Dissection-Endoscopic Mucosal Resection for Large Polyps at the Ileocecal Valve: A Retrospective Single Center Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")