Thomas Jefferson University Hospital Philadelphia, PA
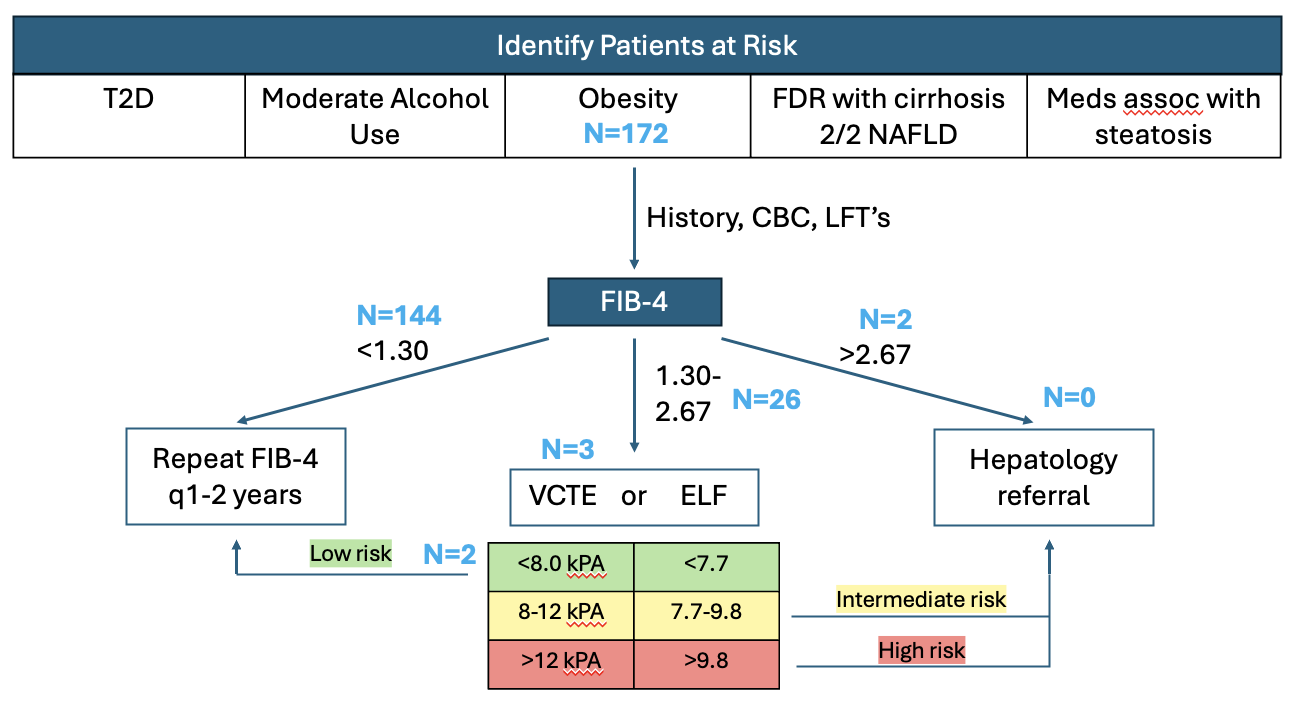
Ananya Venkatesh, MD1, Sanjna Shelukar, MD1, Breanne McDermott, BS2, Julietta Gervase, BA2, Maria Winte, MD1, Rebecca Loh, MD1, Dina Halegoua-DeMarzio, MD1 1Thomas Jefferson University Hospital, Philadelphia, PA; 2Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia, PA Introduction: Metabolic dysfunction- associated steatotic liver disease (MASLD) is a leading cause of chronic liver disease in the United States. Early recognition of MASLD and hepatic fibrosis in the primary care setting is critical for optimal early management. Screening patients at risk of MASLD with the Fibrosis-4 (FIB-4) index is recommended as a first line, non-invasive screening tool for advanced fibrosis. The aim of this study is to determine the rates of MASLD screening in at risk patients and rates of potential advanced fibrosis in an urban resident lead primary care clinic. Methods: A retrospective chart review was conducted in a single internal medicine resident primary care clinic. Patients ages 36- 65 years of age were included and FIB-4 scores were calculated. Patients were stratified into low risk (FIB-4 < 1.3), indeterminate risk (FIB-4 1.3- 2.67), and high risk (FIB-4 >2.67) groups. Secondary risk assessments in the form of elastography orders and hepatology referrals for the indeterminate and high-risk groups, respectively, were assessed. Results: 172 patients with BMI >36 were identified. Of the cohort, 108 were female (63%), and the median age was 53 years. 69% of patients had hypertension, 67% had hyperlipidemia, and 46% had diabetes. 144 patients had a low-risk FIB-4, 26 had an indeterminate-risk FIB-4, and 2 had a high-risk FIB-4. Among the indeterminate risk group, only 3 (12%) patients had an elastography ordered. 2 of these patients completed the test with values of 5.8 and 6.9 kPA. Among the high-risk group, none of the patients were referred to hepatology (Figure 1). Rarely did patients have FIB-4 score noted in their chart. Discussion: Our findings show that previous FIB-4 is rarely being used in the primary care setting, and few patients with indeterminate or high-risk FIB-4 scores are given appropriate secondary workup for MASLD. This stems from underutilization of the FIB-4 index in the primary care setting, which can delay diagnosis leading to progression of fibrosis. Further education of primary care providers is needed to share the importance of utilizing the FIB-4 index during health maintenance screening in patients with metabolic risk factors.
Figure: Figure 1: FIB-4 Screening in Patients with Obesity
Disclosures: Ananya Venkatesh indicated no relevant financial relationships. Sanjna Shelukar indicated no relevant financial relationships. Breanne McDermott indicated no relevant financial relationships. Julietta Gervase indicated no relevant financial relationships. Maria Winte indicated no relevant financial relationships. Rebecca Loh indicated no relevant financial relationships. Dina Halegoua-DeMarzio: 89BIO – Grant/Research Support. Akero – Grant/Research Support. Galectin – Grant/Research Support. Madigral – Advisory Committee/Board Member, Grant/Research Support, Speakers Bureau. Novo Nordisk – Grant/Research Support. Vertex – Advisor or Review Panel Member.
Ananya Venkatesh, MD1, Sanjna Shelukar, MD1, Breanne McDermott, BS2, Julietta Gervase, BA2, Maria Winte, MD1, Rebecca Loh, MD1, Dina Halegoua-DeMarzio, MD1. P3771 - Lost in Stratification: The Underutilization of FIB-4-Guided MASLD Screening in the Primary Care Setting, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.