Dell Medical School at The University of Texas at Austin Austin, TX
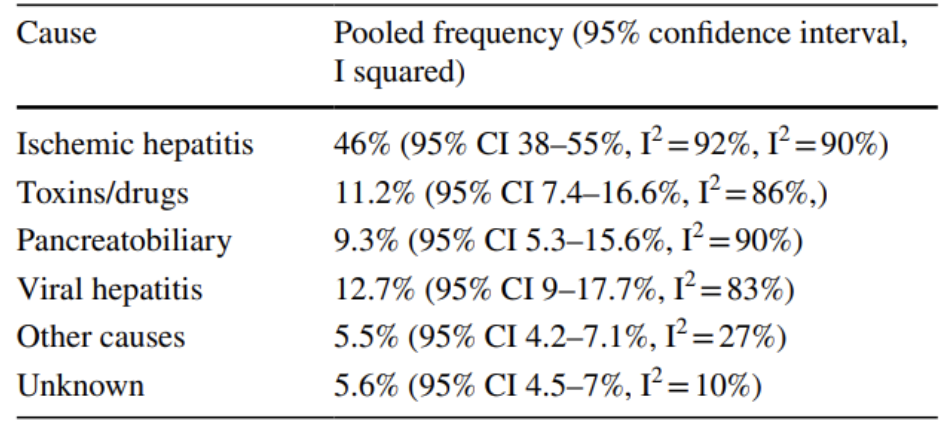
Natalie Malluru, MD1, Darshil Choksi, MD2, Mihir Alexander. Patel, MD, MBA3, Kristina Tzartzeva, MD1 1Dell Medical School at The University of Texas at Austin, Austin, TX; 2University of Texas at Austin Dell Medical School, Austni, TX; 3University of Texas at Austin Dell Medical School, Austin, TX Introduction: Ischemic hepatitis is the leading etiology of marked transaminase elevation in both the general population and patients with cirrhosis, accounting for nearly 50% of such cases¹ (Figure 1). Pericardial tamponade is a rare cause of shock leading to ischemic hepatitis, accounting for less than 2% of cases. We report a rare case of ischemic hepatitis secondary to pericardial tamponade in a patient with end stage renal disease (ESRD) on peritoneal dialysis (PD).
Case Description/
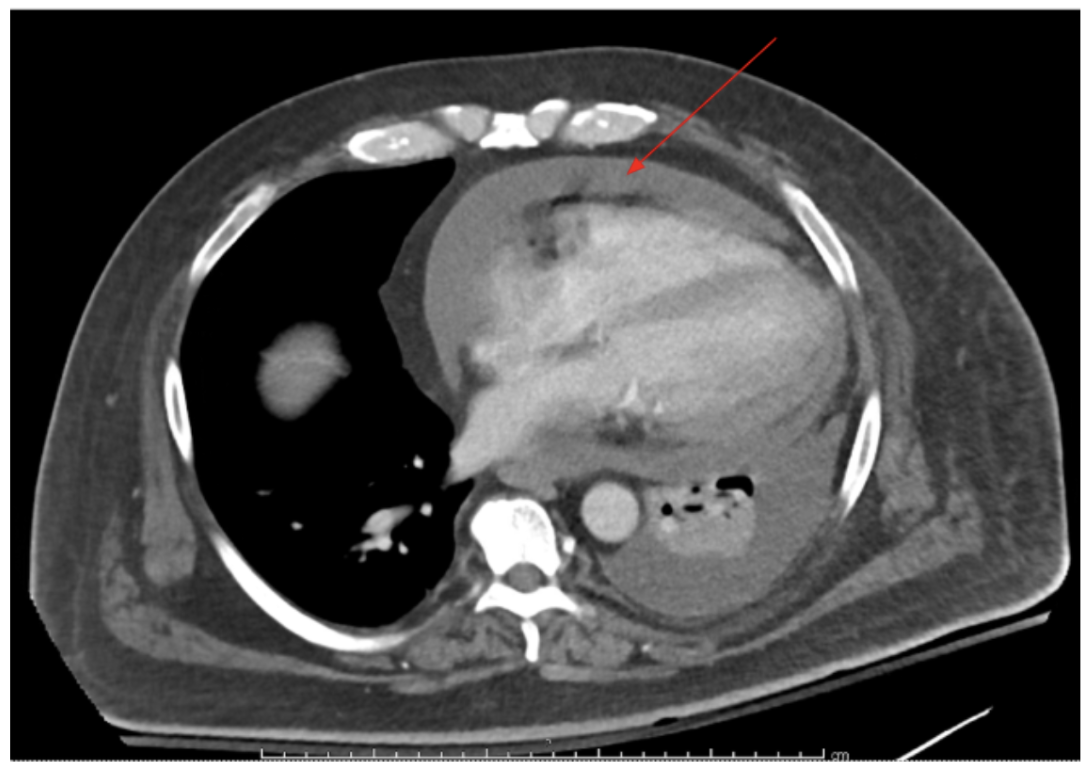
Methods: A 53-year-old man with no known prior liver disease and multiple co-morbidities including ESRD on PD originally presented for a lower extremity wound infection. A few weeks into his hospitalization, he developed an acute rise in transaminases including AST of 1918 and ALTof 585, both of which were normal the day before. Other labs were notable for an INR of 1.58, ALP of 170, total bilirubin of 0.5, and BUN and Cr of 51 and 7.4, respectively. Hemodynamics had been stable. Tylenol level was normal. A liver doppler ultrasound showed patent portal and hepatic veins. Viral hepatitis and autoimmune serologies were negative. Twelve hours after transaminase elevation, a stat CT of the chest, abdomen, and pelvis was ordered to evaluate a new decline in mean arterial blood pressure. Imaging identified a new large pericardial effusion (Figure 2). This was confirmed on echocardiogram, which further showed tamponade physiology. The patient underwent emergent pericardiocentesis with pericardial drain placement, which was ultimately removed after 4 days. Transaminases normalized over the coming days. Discussion: Pericardial effusion and tamponade are known complications of patients receiving dialysis, often due to inadequate dialysis or build up of uremic toxins. Furthermore, patients receiving PD may be at even greater risk due to the unique structural risks associated with PD, such as peritoneo-pericardial fistula formation, that carries a specific risk of dialysate leakage into the pericardium². Although a rare cause of ischemic hepatitis in the general population, pericardial tamponade should be more heavily considered in patients receiving dialysis, particularly peritoneal dialysis.
Figure: Figure 1. Results of a Meta-analysis with pooled frequency of etiologies of marked elevation of liver enzymes to a level > 1,000 international units per liter (IU/L). 1608 patients were included.
Disclosures: Natalie Malluru indicated no relevant financial relationships. Darshil Choksi indicated no relevant financial relationships. Mihir Patel indicated no relevant financial relationships. Kristina Tzartzeva indicated no relevant financial relationships.
Natalie Malluru, MD1, Darshil Choksi, MD2, Mihir Alexander. Patel, MD, MBA3, Kristina Tzartzeva, MD1. P4017 - Under Pressure: A Rare Presentation of Shock Liver Due to Pericardial Tamponade, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.