University of Miami Miller School of Medicine at JFK Medical Center Atlantis, FL
Bebika Subedi, MD, Dipen Dhakal, MD, Panida Charnvitayapong, MD, Amal Benchakroun, MD University of Miami Miller School of Medicine at JFK Medical Center, Atlantis, FL Introduction: Small bowel neuroendocrine tumors (SBNETs) are rare neoplasms derived from midgut neuroendocrine cells, with an annual incidence of 1–2 per 100,000 individuals. Despite their rarity, they have become the most common primary small bowel malignancy, surpassing adenocarcinomas. SBNETs often exhibit an indolent course and variable clinical manifestations, ranging from vague abdominal symptoms to complications like obstruction or bleeding. Their nonspecific presentation can delay diagnosis. Colonoscopy can aid in the diagnosis of SBNETs by allowing direct visualization and biopsy. Early recognition and individualized treatment are essential to optimize outcomes.
Case Description/
Methods: A 55 year female presented with 8–10 weeks of intermittent abdominal pain, bloating, and diarrhea after a presumed food poisoning episode. She denied fever, blood or mucus in stool, flushing or weight loss. She was initially managed conservatively and discharged. Recurrent emergency department visits eventually revealed terminal ileitis and small bowel obstruction (SBO) on imaging. Exam findings included mild abdominal distension, and tachycardia. Labs showed leukocytosis. Despite bowel rest, IV fluids, antibiotics, and corticosteroids, symptoms recurred. Colonoscopy showed nodular inflammation in the terminal ileum, but biopsies were non-diagnostic. After readmission with worsening SBO, surgical exploration revealed a near complete obstruction and mesenteric mass. A right hemicolectomy was performed. Pathology confirmed a 3.4 cm well-differentiated neuroendocrine tumor in the terminal ileum with a 4.9 cm mesenteric mass. Discussion: This case highlights the challenge of diagnosing SBNETs, which often present with vague symptoms and easily mistaken for common gastrointestinal issues. Standard imaging and routine colonoscopy may miss these tumors, especially when they're located deeper or in the terminal ileum. While traditional colonoscopy has some role, emerging techniques offer better diagnostic potential. Tools like video capsule endoscopy provide noninvasive, complete view of the small intestine, while device-assisted enteroscopy, such as double-balloon enteroscopy, allows for direct visualization, biopsy, and even marking of lesions for surgery. In this patient, diagnosis was ultimately made through surgical exploration, but the case underscores the need to incorporate these advanced endoscopic methods earlier, especially when patients present with recurrent, unexplained SBO.
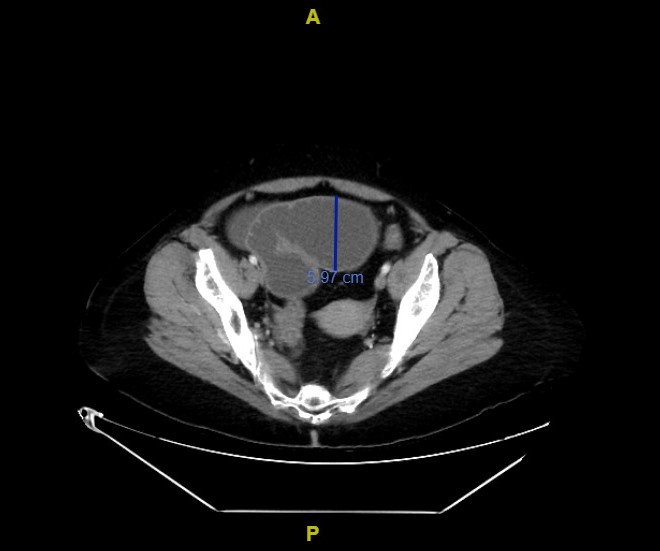
Figure: Small bowel obstruction with small bowel loop measuring up to 5.8 cm.
Figure: Thickened distal ileum with transition point and dilated loops of small bowel.
Disclosures: Bebika Subedi indicated no relevant financial relationships. Dipen Dhakal indicated no relevant financial relationships. Panida Charnvitayapong indicated no relevant financial relationships. Amal Benchakroun indicated no relevant financial relationships.
Bebika Subedi, MD, Dipen Dhakal, MD, Panida Charnvitayapong, MD, Amal Benchakroun, MD. P4099 - Elusive Culprit: Diagnosing Terminal Ileum Neuroendocrine Tumor in a Patient With Recurrent Small Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.