Navin Naik, DO1, Komlan Guedze, MD2, Alexander Kadah, MD1, Farooq Khan, MD3 1Franciscan Health Olympia Fields, Chicago, IL; 2Franciscan Health, Olympia Fields, IL; 3Franciscan Health Olympia Fields, Olympia Fields, IL Introduction: Urachal adenocarcinoma (UA) is a rare subset of bladder cancer. The urachus is a fibrous band that connects the navel to the bladder in a fetus. It typically closes off in the fourth month of development to form the median umbilical ligament, but it can remain open in around a third of adults. While most patent urachus cases are clinically silent, a subset may undergo malignant transformation. This cancer is rare, comprising only 0.01% of all adult cancers and 0.34-0.7% of all bladder cancers. Owing to its insidious onset and non-specific symptomatology, UA is frequently diagnosed at an advanced stage. Although small bowel obstruction (SBO) is a known complication of advanced intra-abdominal malignancy, its association with UA is exceptionally rare. We present a case in which a patient presented with SBO due to metastatic UA.
Case Description/
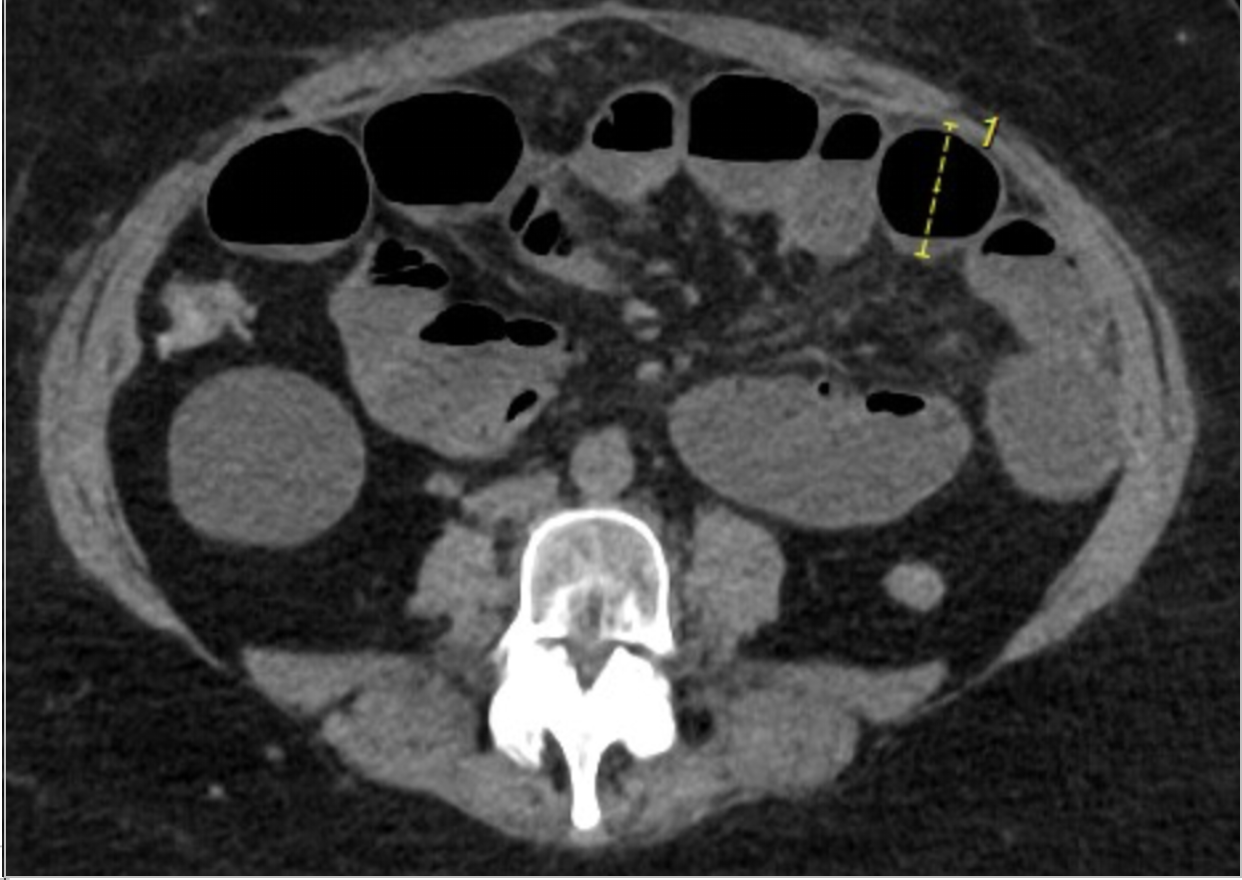
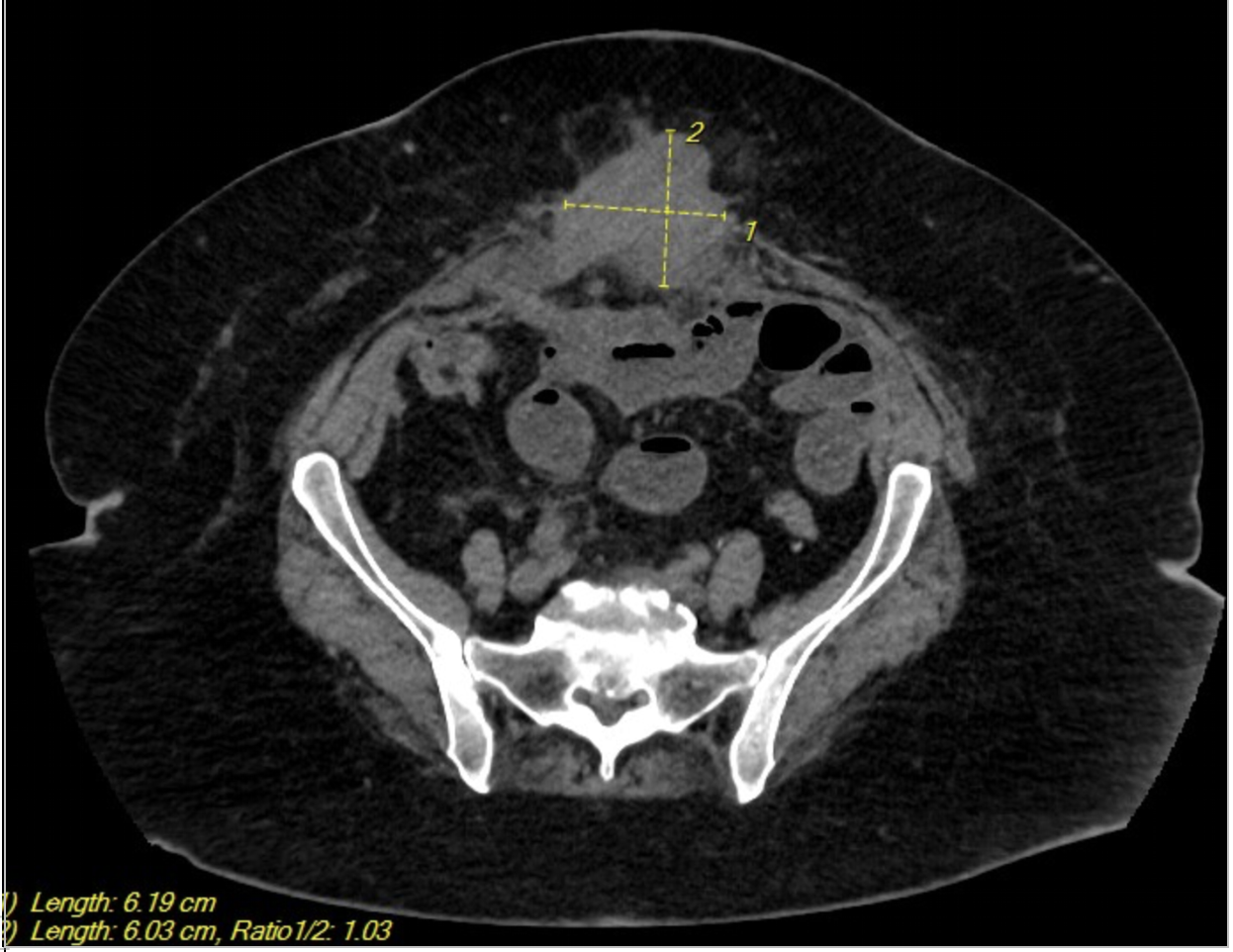
Methods: Our patient is a 57 year old female with a past history of metastatic urachal adenocarcinoma status post partial cystectomy who presented to the emergency department with complaints of abdominal pain and distention, nausea, and vomiting. She also reported that she had not had a bowel movement in several days and was not passing flatulence either. She had previously undergone multiple chemotherapy cycles, including gemcitabine and cisplatin, without a sustained response. One month prior, she was hospitalized with a partial SBO and discharged on total parenteral nutrition. CT scan of her abdomen and pelvis during present admission was obtained and showed dilated loops of small bowel consistent with obstruction, as well as re-demonstration of her known solid mass (Image 1,2). A malignant etiology of her SBO was presumed, given the patient’s oncologic history and disease progression. Given her advanced disease, surgery was not a viable option and she refused nasogastric tube insertion. The decision was made to transition to hospice care and she was discharged home. Discussion: This case underscores the aggressive nature of UA and its potential to cause life-threatening complications such as SBO. While SBO is frequently encountered in surgical and oncologic contexts, its occurrence secondary to UA is exceedingly rare and poorly described in the literature. Management is often palliative in widespread metastasis, as was the case here. Given the diagnostic challenges and limited treatment options, early recognition and multidisciplinary management are imperative. Further research is warranted to optimize therapeutic strategies for this rare malignancy.
Figure: Image 1: Dilated loops of small bowel with air-fluid levels consistent with SBO
Figure: Image 2: Known solid mass lesion consistent with malignancy in the anterior abdominal wall
Disclosures: Navin Naik indicated no relevant financial relationships. Komlan Guedze indicated no relevant financial relationships. Alexander Kadah indicated no relevant financial relationships. Farooq Khan indicated no relevant financial relationships.
Navin Naik, DO1, Komlan Guedze, MD2, Alexander Kadah, MD1, Farooq Khan, MD3. P4094 - From Bladder to Blockage: Urachal Adenocarcinoma Presenting With Small Bowel Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.