Venkat Arutla, MD, Nathan P. Heller, MD, Kevin Casey, MD Rochester General Hospital, Rochester, NY Introduction: Abdominal pain is a very common chief complaint that is often dependent on age, gender, or accompanying symptoms. Arriving at the correct diagnosis entails an astute clinician, laboratory data, and often requires imaging. Here, we discuss a diagnosis for abdominal pain appearing several decades after the age of typical presentation.
Case Description/
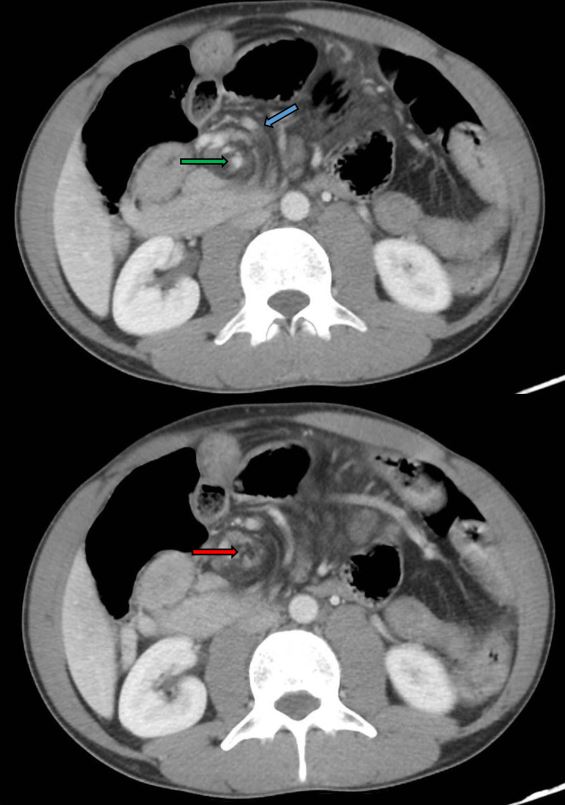
Methods: A 34-year-old male with past medical history of irritable bowel syndrome diarrhea subtype (IBS-D), gastroesophageal reflux disease, umbilical and inguinal hernia repair, presented to the hospital with complaints of abdominal pain, associated with nausea, vomiting and reduced number of bowel movements (BM) compared to baseline. The pain and number of BMs were deviations from his baseline. The patient underwent a computed tomography (CT) scan of his abdomen and pelvis and was found to have multiple dilated loops of small bowel with air-fluid levels and a transition point, with swirling and edematous changes of the mesentery suggestive of an internal hernia (Figure 1). The scan also revealed an abrupt occlusion of the superior mesenteric artery (SMA). CT-Angiography of the abdomen and pelvis redemonstrated swirling of the mesentery, resulting in compression of superior mesenteric vein branches and a new finding of an abnormal mesenteric collateral vein formation anterior to the right kidney. The patient underwent diagnostic laparoscopy and was found to have bowel obstruction secondary to a 3-4cm left posterior mesenteric defect, medial to the ligament of Treitz, consistent with a left para-duodenal hernia. Due to an unsuccessful laparoscopic approach, he underwent open hernia reduction and closure of the mesenteric defect. Discussion: Hernias are a common cause of abdominal pain; however, congenital internal hernias (CIH) are rarer and pose a clinical and radiological diagnostic challenge. Congenital bowel malrotation (CBM) is usually due to abnormal embryogenic development resulting in rotation of the midgut around the SMA, as potentially seen with the patient’s initial CT scan. CIHs, such as paraduodenal hernias, can occur as a result of CBM due to abnormal mesenteric defects. CIHs are usually diagnosed in the neonatal and early childhood period, making presentation in adulthood relatively rare. Swift recognition of “swirl” pattern on imaging, along with a clinical picture of abdominal pain and decreased bowel movements should prompt clinicians to consider congenital internal hernias and early surgical intervention.
Figure: Figure 1: CT Abdomen and Pelvis showing swirling of mesentery (blue arrow), patent SMA (green arrow) and occluded SMA (red arrow).
Disclosures: Venkat Arutla indicated no relevant financial relationships. Nathan Heller indicated no relevant financial relationships. Kevin Casey indicated no relevant financial relationships.
Venkat Arutla, MD, Nathan P. Heller, MD, Kevin Casey, MD. P4089 - A Simple Twist of Fate: Untying the Knots of Abdominal Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.