Mina Ayad, MD1, Gautam Anand, MD1, Keshavi Mahesh, MD1, Hootan Vakili, MD1, Aryama Sharma, MD2, Jose Lisandro Gonzalez Martinez, MD1 1Broward Health North, Pompano Beach, FL; 2Broward Health North, Deerfield Beach, FL Introduction: Foreign body (FB) ingestion in adults without recollection is rare, especially in those with altered gastrointestinal anatomy such as post–sleeve gastrectomy (SG) patients. These cases present diagnostic challenges and are prone to delayed recognition. Persistent symptoms in such patients warrant careful evaluation and repeat imaging to avoid serious complications.
Case Description/
Methods: A 57-year-old woman with a history of SG four years prior presented with two weeks of persistent right upper quadrant (RUQ) abdominal pain. The pain began with diarrhea, which resolved, and she denied nausea, vomiting, or chills. The pain worsened when lying flat and improved with upright positioning.
Initial CT imaging at an outside hospital revealed a hiatal hernia with gastritis. Despite this, her pain intensified, prompting further evaluation. Repeat imaging identified a foreign body—suspected to be a bone fragment—lodged in the fourth portion of the duodenum, with surrounding inflammation concerning for microperforation. The patient denied ingesting any foreign material and specifically denied recent chicken consumption. Physical exam showed increasing RUQ tenderness, low-grade fever, and leukocytosis, suggesting worsening inflammation.
GI was consulted for urgent evaluation. Small bowel enteroscopy confirmed a sharp FB embedded in the distal duodenum. It was successfully removed using large-capacity forceps and a protective hood. Following removal, the patient’s symptoms resolved, and her clinical condition stabilized. Discussion: This case illustrates the complexity of diagnosing FB ingestion in adults with altered GI anatomy. Post-SG patients may present with vague or atypical symptoms, and the absence of an ingestion history can delay diagnosis. Persistent unexplained abdominal pain in this population should prompt further imaging, even after an initially unremarkable workup.
The identification of a bone fragment causing microperforation underscores the importance of maintaining a high index of suspicion. Early endoscopic intervention enabled prompt treatment, avoided surgical complications, and led to full recovery. In post-bariatric patients with persistent abdominal symptoms, FB ingestion should remain on the differential—even without patient recollection.
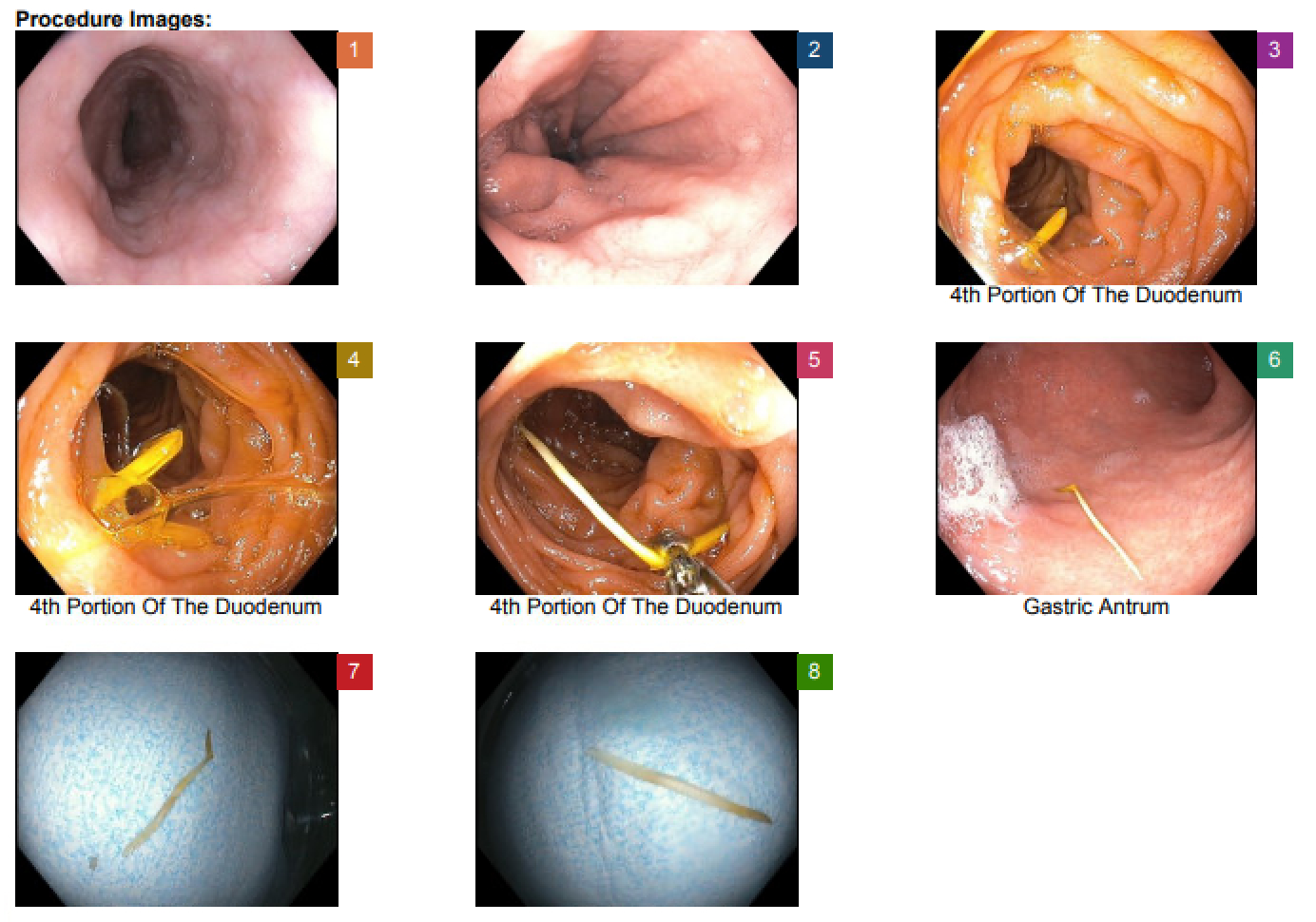
Figure: 1. Normal esophagus view, confirming no abnormalities in the upper GI tract.
2. Progression through the upper GI tract showing normal mucosal patterns.
3. Foreign body (a chicken bone fragment) visualized in the fourth portion of the duodenum.
4. Closer view of the foreign body lodged in the fourth portion of the duodenum.
5. The foreign body is engaged with large-capacity forceps for removal.
6. Further view of the foreign body in the gastric antrum during retrieval.
7. Foreign body visualized after extraction, likely a bone fragment.
8. Final image of the extracted foreign body post-removal, confirming successful retrieval.
Disclosures: Mina Ayad indicated no relevant financial relationships. Gautam Anand indicated no relevant financial relationships. Keshavi Mahesh indicated no relevant financial relationships. Hootan Vakili indicated no relevant financial relationships. Aryama Sharma indicated no relevant financial relationships. Jose Lisandro Gonzalez Martinez indicated no relevant financial relationships.
Mina Ayad, MD1, Gautam Anand, MD1, Keshavi Mahesh, MD1, Hootan Vakili, MD1, Aryama Sharma, MD2, Jose Lisandro Gonzalez Martinez, MD1. P4163 - The Mystery Bone: Unrecalled Foreign Body Causing Right Upper Quadrant Pain Post-Sleeve Gastrectomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.