Supritha Chintamaneni, MBBS1, Bilal Ashraf, MD2, Aakriti Soni, MD3, Galvin S. Dhaliwal, MD3, Guha Sushovan, MD1 1HCA Healthcare, Kingwood, TX; 2HCA Healthcare Kingwood Hospital/University of Houston, Kingwood, TX; 3HCA Healthcare Kingwood Hospital/University of Houston, Houston, TX Introduction: B-lymphoblastic leukemia/lymphoma (B-ALL) is an aggressive hematologic malignancy that primarily affects the bone marrow and peripheral blood, but can occasionally involve extramedullary sites such as the central nervous system, testicles, and more rarely, the gastrointestinal (GI) tract. When the GI system is involved, it presents with abdominal pain, nausea, vomiting, or bleeding mimicking primary GI malignancies, often delaying accurate diagnosis. This case highlights a rare presentation of B-ALL with gastric involvement.
Case Description/
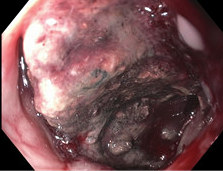
Methods: A 35-year-old male with history of hypertension, type 2 diabetes mellitus, and chronic alcohol use presented to the emergency department with nausea, intractable vomiting, episodes of bloody stools, and 100-pound unintentional weight loss over seven months. A CT scan of the abdomen and pelvis revealed numerous small lucent lesions in both the appendicular and axial skeleton. Given the significant weight loss, hemoglobin of 9 g/dL, GI symptoms, and imaging findings, an esophagogastroduodenoscopy was performed. It revealed a large, ulcerated, circumferential mass in the gastric antrum with necrosis and recent bleeding, raising concern for primary gastric malignancy. Multiple biopsies were taken, hematology was consulted, and a bone marrow biopsy was performed.
Bone marrow analysis showed 87% B-lymphoblasts, and flow cytometry (CD10+, CD19+, CD34+, TdT+ B-lymphoblasts) confirmed B-ALL. Peripheral smear demonstrated circulating blasts, severe thrombocytopenia, and anemia. Cytogenetic testing identified CRLF2 overexpression and IKZF1 deletion—both associated with poor prognosis. Gastric biopsy confirmed the mass was B-ALL infiltration rather than primary gastric carcinoma, consistent with marrow findings. The patient was started on proton pump inhibitors and transferred for higher-level hematology care. Discussion: The mechanism of gastric infiltration in B-ALL is not well understood, though rare cases of GI involvement have been reported. Imaging plays a critical role in identifying extramedullary disease, especially during relapse after targeted therapies like blinatumomab or inotuzumab ozogamicin. NCCN guidelines recommend comprehensive evaluation, including imaging, when extramedullary spread is suspected. The growing role of CAR T-cell therapy, including tisagenlecleucel, in treating relapsed or refractory B-ALL with extramedullary manifestations underscores the importance of early hematologic evaluation for timely diagnosis and optimal outcomes.
Figure: Mass in gastric antrum.
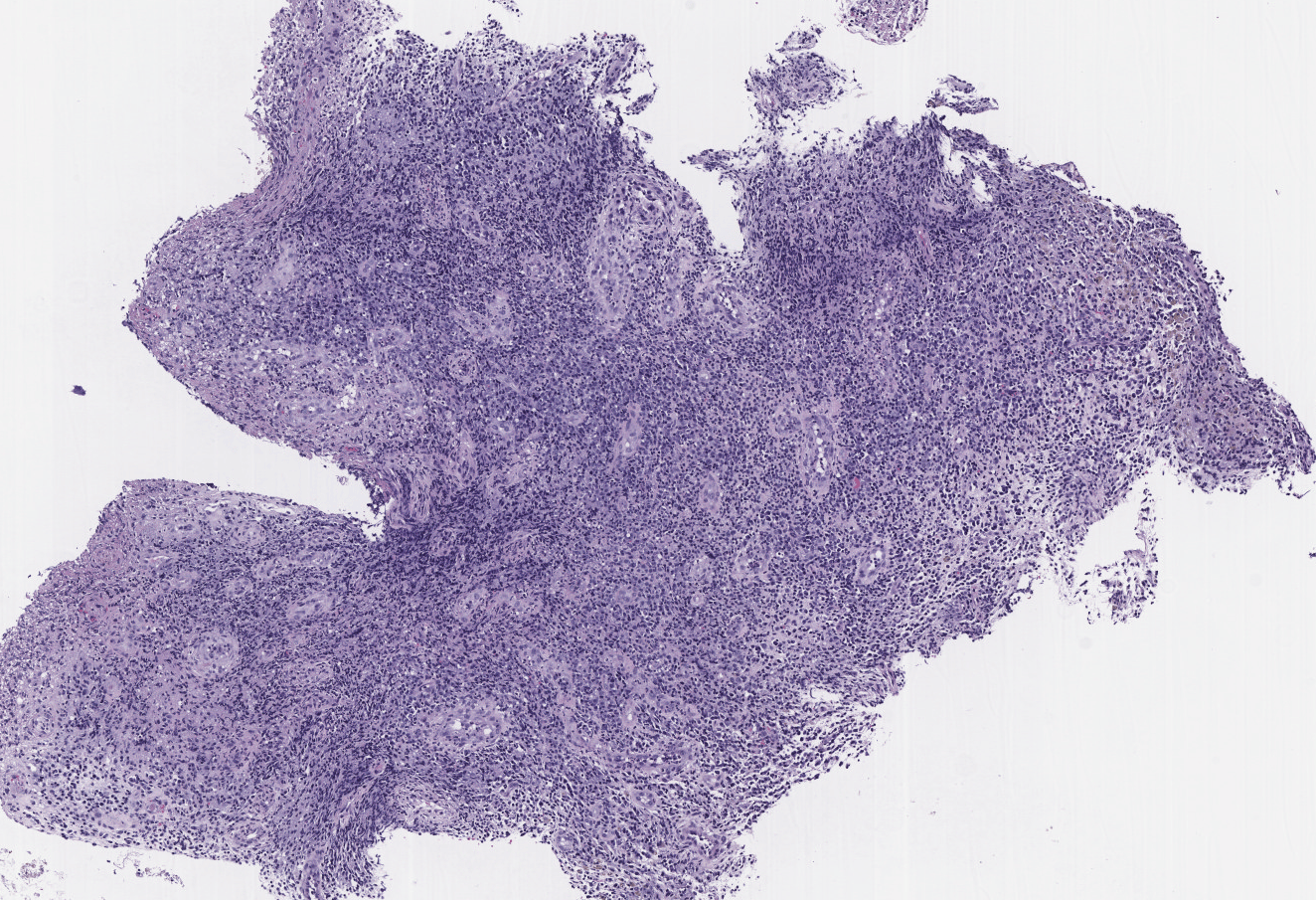
Figure: Intermediate power images of the stomach biopsy shows predominantly granulation tissue with scattered atypical TdT positive cells, consistent with involvement of B-lymphoblastic leukemia/lymphoma.
Disclosures: Supritha Chintamaneni indicated no relevant financial relationships. Bilal Ashraf indicated no relevant financial relationships. Aakriti Soni indicated no relevant financial relationships. Galvin Dhaliwal indicated no relevant financial relationships. Guha Sushovan indicated no relevant financial relationships.
Supritha Chintamaneni, MBBS1, Bilal Ashraf, MD2, Aakriti Soni, MD3, Galvin S. Dhaliwal, MD3, Guha Sushovan, MD1. P4229 - When Leukemia Takes a Bite: Unusual Gastric Involvement in B-ALL, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.