Vaishnavi K. Modi, MD1, Mahader N. Wossene, MD2, Taylor Zak, MD, PhD3, Anum Nawaz, MBBS, MD1, Aashutosh Sah, MD1, Zohaib Haque, DO4 1MacNeal Hospital Loyola Medicine, Oak Park, IL; 2MacNeal Hospital Loyola Medicine, Berwyn, IL; 3Loyola University Medical Center, Maywood, IL; 4MacNeal Hospital Loyola Medicine, Chicago, IL Introduction: Gastric diffuse large B-cell lymphoma (DLBCL) is a rare and aggressive subtype of non-Hodgkin lymphoma, accounting for ~ 1.5% of gastric malignancies and ~10% of lymphomas. Clinical symptoms—such as anemia, weight loss, and early satiety—are often nonspecific and may mimic benign gastrointestinal (GI) conditions like gastritis or diabetic gastroparesis. Gastroparesis has been associated with gastric lymphoma in rare cases, with fewer than 50 reported. Early endoscopy with biopsy is crucial, as delayed diagnosis can affect prognosis. We report an atypical presentation of gastric DLBCL in a high-risk patient, emphasizing the need for broad differential diagnosis.
Case Description/
Methods: A 65-year-old male with uncontrolled diabetes mellitus and hypertension presented with chronic fatigue, generalized weakness, intermittent headaches, and an unintentional 10-pound weight loss over two weeks. Six months earlier, he had undergone esophagogastroduodenoscopy (EGD) for persistent nausea and vomiting, which revealed esophagitis and mild to moderate gastritis; biopsies showed GE junction metaplasia without dysplasia.
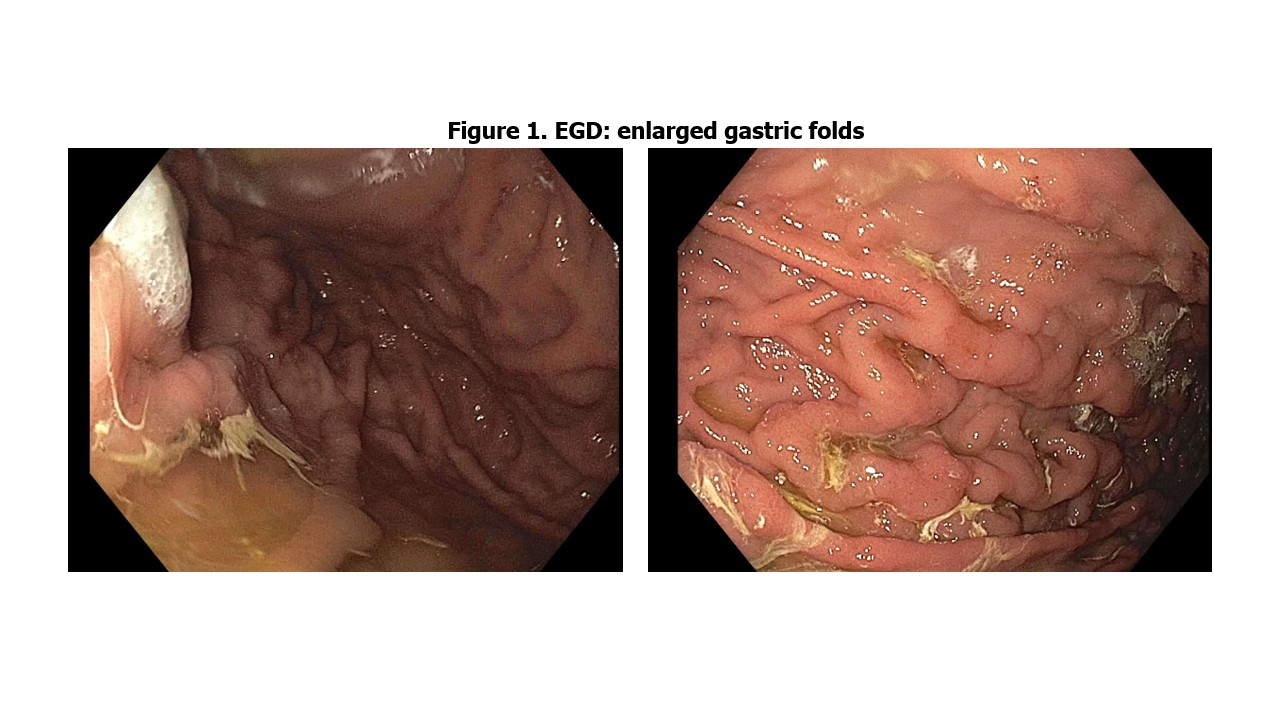
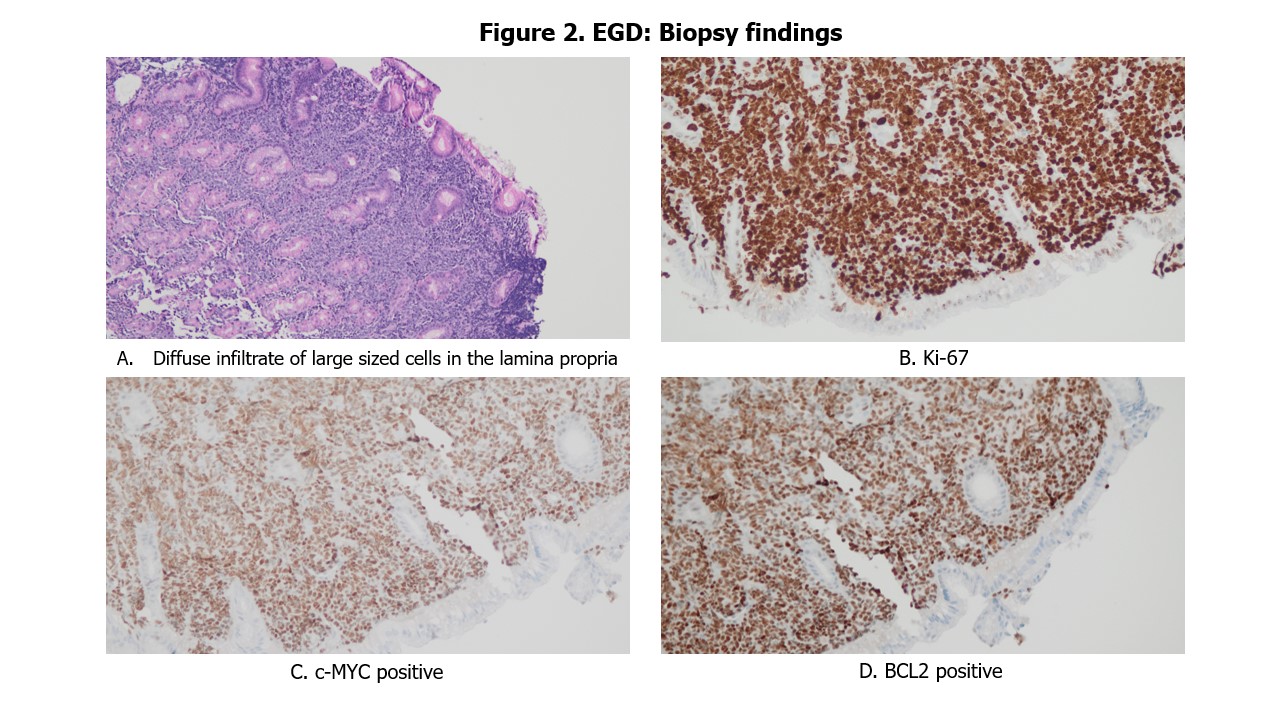
On current admission, laboratory tests revealed severe iron deficiency anemia; the remainder workup was unremarkable. A gastric emptying study showed delayed gastric emptying, which was attributed to long-standing diabetes, and he was started on metoclopramide. Due to ongoing symptoms and concern for underlying malignancy, colonoscopy was performed but was negative. A repeat EGD demonstrated erosive gastritis and enlarged gastric folds (Figure 1). Biopsy revealed diffuse large B-cell lymphoma (Figure 2A), with FISH testing positive for MYC and BCL2 rearrangements (Figure 2C, 2D), confirming a diagnosis of "Double Hit Lymphoma." The patient elected for home hospice care. Discussion: This case highlights the diagnostic challenge of gastric DLBCL, particularly in patients with comorbidities (diabetes), where symptoms may mimic benign GI disorders. Persistent findings such as weight loss and anemia should prompt further investigation. In this case, repeat endoscopy and biopsy confirmed DLBCL with MYC and BCL2 rearrangements, consistent with Double Hit Lymphoma—an aggressive variant with poor prognosis requiring timely management. Early stages can be managed with regimens like R-EPOCH, with a 67% two-year event-free survival rate, emphasizing the importance of clinical suspicion and early tissue diagnosis in high-risk patients.
Figure: Figure 1. EGD findings.
Figure: Figure 2. EGD Biopsy findings.
Disclosures: Vaishnavi Modi indicated no relevant financial relationships. Mahader Wossene indicated no relevant financial relationships. Taylor Zak indicated no relevant financial relationships. Anum Nawaz indicated no relevant financial relationships. Aashutosh Sah indicated no relevant financial relationships. Zohaib Haque indicated no relevant financial relationships.
Vaishnavi K. Modi, MD1, Mahader N. Wossene, MD2, Taylor Zak, MD, PhD3, Anum Nawaz, MBBS, MD1, Aashutosh Sah, MD1, Zohaib Haque, DO4. P4277 - Looking Deeper: A Case of Double HIT Gastric Lymphoma Masquerading as Gastroparesis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")