Shradha Gupta, MD1, Navroop Nagra, MD2, Gavin Levinthal, MD3 1HonorHealth, Chandler, AZ; 2HonorHealth, Scottsdale, AZ; 3Honor Health Gastroenterology - SCOTTSDALE, AZ, Scottsdale, AZ Introduction: Acute gastric volvulus (AGV) is a rare condition associated with a very high mortality rate of 30-50%. Early diagnosis and prompt management are key for improving patient outcomes. We present a case of gastric volvulus which was resolved after the upper endoscopy.
Case Description/
Methods: A 60-year-old man with no significant past medical history presented with a 2-day history of epigastric abdominal pain and multiple episodes of non- bloody vomiting. Upon initial evaluation, he was hemodynamically stable. Computed tomography (CT) scan of the abdomen/pelvis revealed paraoesophageal hernia, gastric outlet obstruction secondary to gastric volvulus. A nasogastric tube was placed and was found to be positioned in the proximal stomach.
The patient underwent an esophagogastroduodenoscopy (EGD) revealing a large hiatal hernia and LA grade B esophagitis. A gastric twist was encountered, but the scope was successfully advanced into the distal stomach which was located in the thoracic cavity. Upon examination, the mucosa in the distal stomach exhibited signs of ischemia with slightly bluish discoloration and hematin, but no ischemic ulcers were seen. Upon withdrawal, the stomach was observed to have untwisted indicating resolution of the gastric volvulus which was confirmed on upper GI series done post procedure.
Following discussion of the treatment options, the patient elected to defer surgical repair of the paraoesophageal hernia and was discharged home in stable condition. Discussion: Acute gastric volvulus is a potentially life-threatening condition that may lead to gastric ischemia or perforation, associated with high mortality. The Borchardt's Triad of gastric volvulus, described by Borchardt in 1904, consists of severe epigastric pain, retching without vomiting, and inability to pass a nasogastric tube. Emergent surgical management should be prompted for unstable patients to improve patient outcomes. Recurrence is high, and surgery is definite treatment, but endoscopy can be done to relieve acute obstruction.
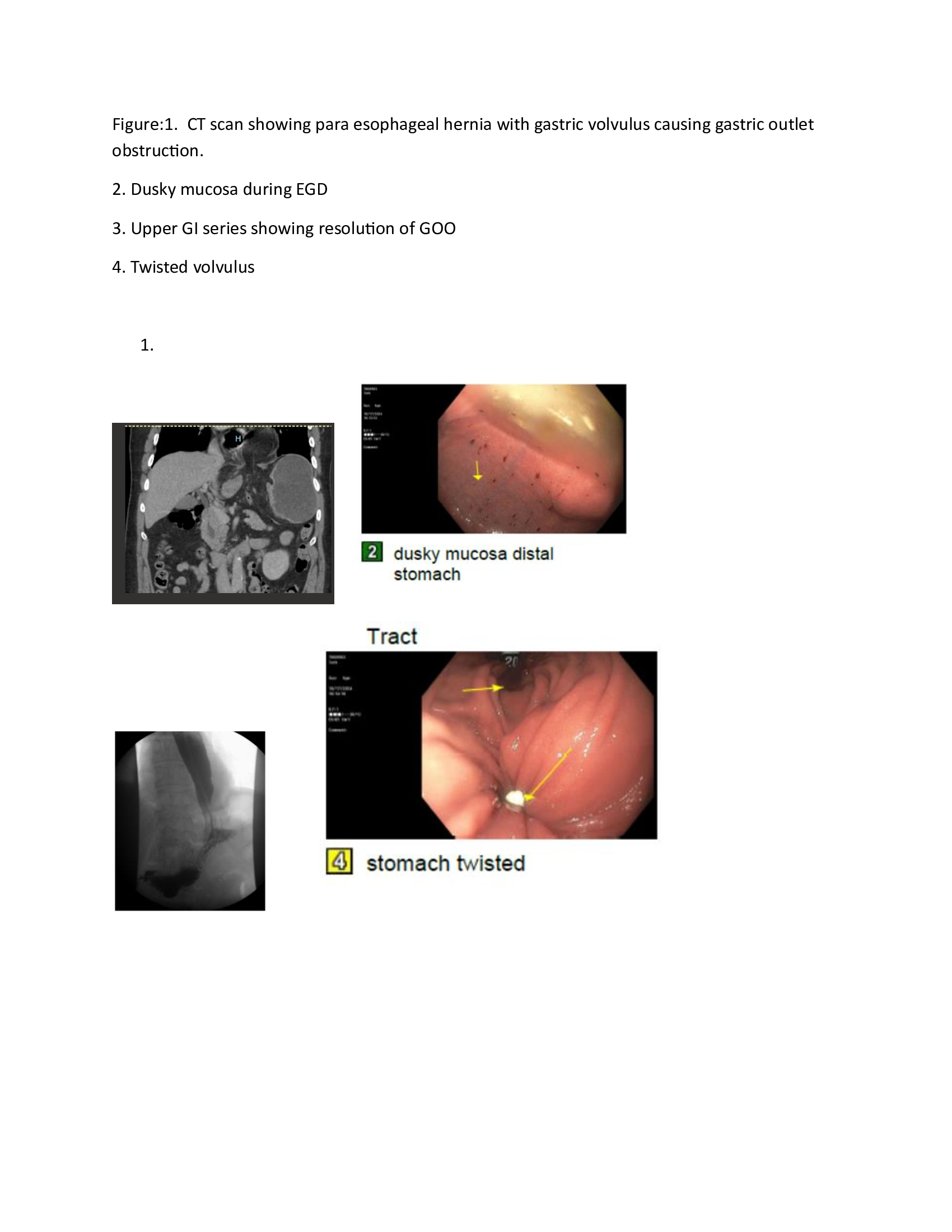
Figure: Figure:1. CT scan showing para esophageal hernia with gastric volvulus causing gastric outlet obstruction. 2. Dusky mucosa during EGD 3. Upper GI series showing resolution of GOO 4. Twisted volvulus
Disclosures: Shradha Gupta indicated no relevant financial relationships. Navroop Nagra indicated no relevant financial relationships. Gavin Levinthal indicated no relevant financial relationships.
Shradha Gupta, MD1, Navroop Nagra, MD2, Gavin Levinthal, MD3. P4274 - The Twist Resolves: Successful Endoscopic Manage of Gastric Volvulus Causing Gastric Outlet Obstruction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Shradha Gupta, MD photo")