Sabrine Sleem, DO1, Mariam Sleem, OMS-IV2, C. Whalen Clark, MD3 1Arnot Ogden Medical Center, Horseheads, NY; 2Alabama College of Osteopathic Medicine, Wesley Chapel, FL; 3Florida Medical Clinic, Tampa, FL Introduction: Gastric Diverticula are the rarest of gastrointestinal diverticula. Prevalence ranges from 0.04% in contrasted radiography studies and 0.01% to 0.11% at EGD (1). Congenital gastric diverticula are true diverticula; they contain all layers of the stomach wall. Acquired gastric diverticula are pseudodiverticula; pulsion-type herniation through the gaps in the muscular layer of the gastric wall (7). Gastric diverticula are most commonly congenital, located in the fundic region (2). Acquired gastric diverticula are hardly ever observed, typically located in antrum, and occur concurrently with other gastric pathology (1). CT scan will reveal a well-defined saccular collection of gas or fluid that demonstrates communication with the gastric cavity often seen as filling with iodinated oral contrast (3). This case highlights clinical manifestations, diagnostic considerations, and management of gastric diverticula.
Case Description/
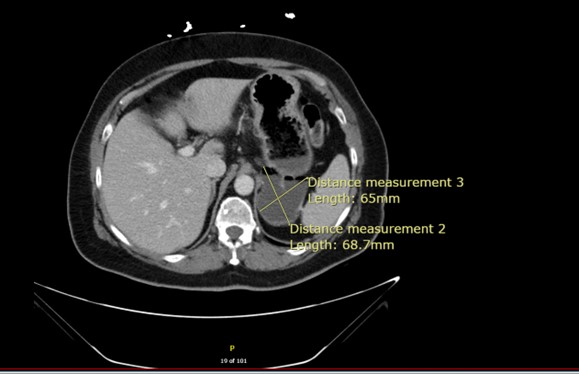
Methods: 62-year-old female with history of GERD, migraines, and HTN presented with abdominal pain, chest pressure, regurgitation, frequent eructation with foul odor, and early satiety of 4 months duration. EGD revealed a medium sized “paraesophageal hernia.” She was referred to general surgery for further management. CTAP completed 2 months prior was reviewed along with recent EGD. CT displayed a 7 cm posterior gastric diverticulum. She underwent robotic partial gastrectomy with resection of the gastric diverticulum in the fundus. Intraoperatively, EGD confirmed successful resection of the diverticulum along with discovery of phytobezoar. 2 weeks post op, symptoms of eructation resolved with improvement in abdominal pain. Pathology exhibited saccular unremarkable gastric oxyntic mucosa-lined pouch, consistent with acquired diverticulum, negative for significant diverticulitis, mucosal inflammation, mass lesion, neoplasia, or malignancy. She was placed on diet avoiding high cellulose foods and prescribed Enzymatica ™ daily to aid digestion. Discussion: This case demonstrates an unusual gastric diverticulum in setting of undiagnosed gastroparesis with phytobezoar. Pathology supports an acquired diverticulum. The coexistence of chronic GERD and gastroparesis raises the possibility that altered gastric motility and raised intragastric pressure were pathophysiologic drivers in the development and progression of the diverticulum. This case depicts the need to consider motility disorders as potential etiologic contributors of symptomatic gastric diverticula.
Figure: CT of the Abdomen depicting the gastric diverticulum
Disclosures: Sabrine Sleem indicated no relevant financial relationships. Mariam Sleem indicated no relevant financial relationships. C. Whalen Clark indicated no relevant financial relationships.
Sabrine Sleem, DO1, Mariam Sleem, OMS-IV2, C. Whalen Clark, MD3. P4267 - Rare Case of Gastric Diverticulum: Unique Pathology in a 62-Year-Old Female, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.