University of Chicago Northshore Internal Medicine Evanston, IL
Madhav Patel, DO1, Ushan Ranasinghe, MD2, Farhan Quader, MD3 1University of Chicago, NorthShore Internal Medicine, Evanston, IL; 2University of Chicago, NorthShore Gastroenterology, Evanston, IL; 3Endeavor Health Gastroenterology, Evanston, IL Introduction: Gastrointestinal (GI) metastases from breast cancer are rare and typically occur in patients with known/recurrent disease. Nonspecific symptoms, such as nausea, vomiting, dysphagia, and weight loss, can lead clinicians to pursue functional or benign causes. This diagnostic uncertainty can delay the identification of malignant GI involvement. Pyloric stenosis (PS) in adults is most frequently attributed to PUD or GI malignancy; however, extrinsic compression or mural infiltration from metastatic disease should also be considered.
Case Description/
Methods: A 67-year-old woman with a history of HLD presented with a 1-year history of progressive dysphagia and unintentional 20-pound weight loss. She denied additional GI symptoms. Initial EGD revealed a benign-appearing PS with retained gastric contents; the stenosis precluded scope passage. A repeat EGD six weeks later demonstrated persistent PS. Dilation was performed and biopsies were obtained. Histology showed adenocarcinoma with lobular carcinoma-like morphology, positive for PAN-CK, GATA3, and estrogen receptor, and negative for lymphoid markers, consistent with a breast primary.
Despite a negative mammogram one year prior which showed only stable benign calcifications, new targeted breast imaging revealed a 9 mm irregular mass in the right breast and an enlarged right axillary lymph node. US-guided biopsy confirmed invasive ductal carcinoma, estrogen receptor–positive, progesterone receptor–negative, HER2-negative. Staging imaging demonstrated metastases to the ribs, spine, femur, and omentum. The patient was initiated on hormone and targeted therapy. Following pyloric dilation, she reported significant improvement in dysphagia. Discussion: This case highlights a rare presentation of metastatic breast cancer manifesting as PS in a patient without a prior cancer diagnosis. Unlike typical presentations, which occur years after breast cancer diagnosis or during relapse, this patient’s GI findings preceded cancer detection. Endoscopy with biopsy was crucial for both diagnosis and symptom relief.
Due to the submucosal location of many GI metastases, superficial biopsies may yield false negatives. Diagnostic yield can be improved with deeper biopsies or endoscopic US–guided sampling. Despite its rarity, metastatic disease should remain in the differential for adult-onset PS, especially when symptoms are unexplained by common etiologies. Early recognition can lead to timely management and intervention, improving both outcomes and quality of life.
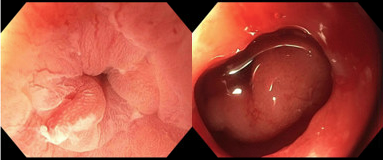
Figure: EGD images revealing pyloric stenosis before (2mm) and after (11mm) pyloric balloon dilation.
Madhav Patel, DO1, Ushan Ranasinghe, MD2, Farhan Quader, MD3. P4263 - Adult-Onset Pyloric Stenosis as the Initial Presentation of Metastatic Breast Cancer, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Madhav Patel, DO photo")