Peter Senada, MD, Yusuke Hashimoto, MD University of Florida College of Medicine, Jacksonville, FL Introduction: Although the prevalence of gastric cancer had decreased over the last decades, gastric polyps are increasingly common. Most polyps are non-neoplastic and don’t require treatment, however, some polyps have a higher risk of malignancy or are cancerous at the time of diagnosis. These polyps are usually associated with H. pylori infection or arise on top of inflammatory polyps. We present a rare case of gastric adenocarcinoma on top of a seemingly benign large polyp
Case Description/
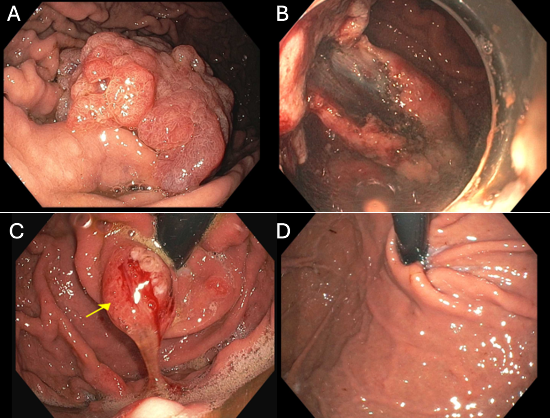
Methods: A 62 y.o. male with history of CAD, HTN and HLD presented to the Gastroenterology clinic for evaluation of chronic GERD. Reports being on anti-reflux medication since age 15. Denied any nausea or vomiting, weight loss or bleeding. No family history of gastric cancer. Had normal upper endoscopy 7 years ago. He underwent EGD and a single > 80 mm pedunculated frond-like/villous and polypoid mass with no bleeding was found on the greater curvature of the stomach(A). Biopsies showed superficial fragments of adenomatous polyp. He underwent endoscopic submucosal dissection(B) of the polyp through injection of 5 mL of Orise gel, circumferential incision around the lesion into the submucosa was performed with an insulated tip knife, the stalk was dissected from the underlying deep layers with the electrocautery SB and IT knife with complete resection and no bleeding. 3 hemostatic clips were placed to prevent bleeding after resection. Pathology found adenomatous polyp with high-grade dysplasia and few foci of adenocarcinoma, favor intramucosal, with no lymphovascular or perineural invasion
A 3 months surveillance EGD showed healthy post resection scar with one clip, biopsies showed gastric mucosa with reactive changes and no tumor seen. Another 20mm erosive polyp at the cardia was found and biopsied(C). This was a polypoid gastric mucosa with hyperplastic changes. Random gastric biopsies were negative for H. pylori. Multiple repeat EGDs were done afterwards with no evidence of recurrence of the resected polyp or any malignancy in the stomach. The cardiac polyp also showed spontaneous disappearance(D) Discussion: Distinguishing neoplastic gastric polyps endoscopically and morphologically remains challenging. A thorough endoscopic evaluation is crucial in identifying polyps with high risk for malignancy. Early recognition and intervention when appropriate are critical to improving patient outcomes, decreasing both morbidity and mortality rate. We report a case of the gastric polyps with pathological assessment and insights
Figure: (A) Large gastric polyp. (B) Submucosal dissection of the polyp. (C) Cardiac polyp. (D)Resolution of polyp
Disclosures: Peter Senada indicated no relevant financial relationships. Yusuke Hashimoto indicated no relevant financial relationships.
Peter Senada, MD, Yusuke Hashimoto, MD. P4246 - To Resect or Not to Resect? Story of a Large Gastric Polyp!, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.