Shiab Mussad, MD1, Jai Kumar, MD2, Serge Sorser, MD3 1Henry Ford Providence Hospital, Dearborn, MI; 2Wayne State University School of Medicine / Ascension Providence Rochester Hospital, Rochester, MI; 3Henry Ford Health, Southfield, MI Introduction: Breast cancer is the most common cancer in females, with invasive lobular carcinoma (ILC) accounting for 10-15% of all breast cancers. Gastrointestinal involvement is most common with the ILC subtype, but metastasis remains rare and is diagnosed in only up to 0.5% of patients. However, autopsy studies report gastric involvement in 8-15% of cases, suggesting significant clinical underdiagnosis.
Case Description/
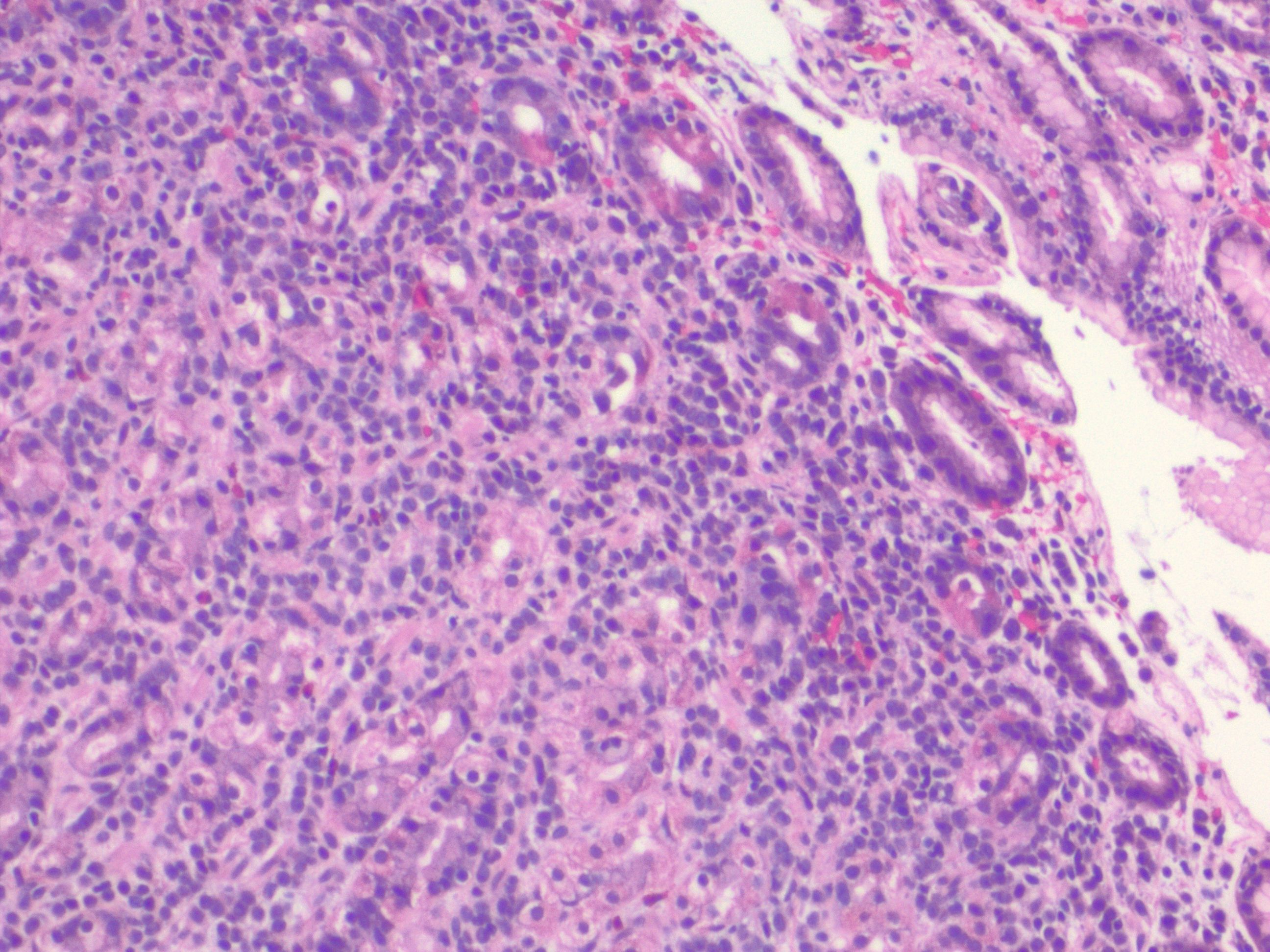
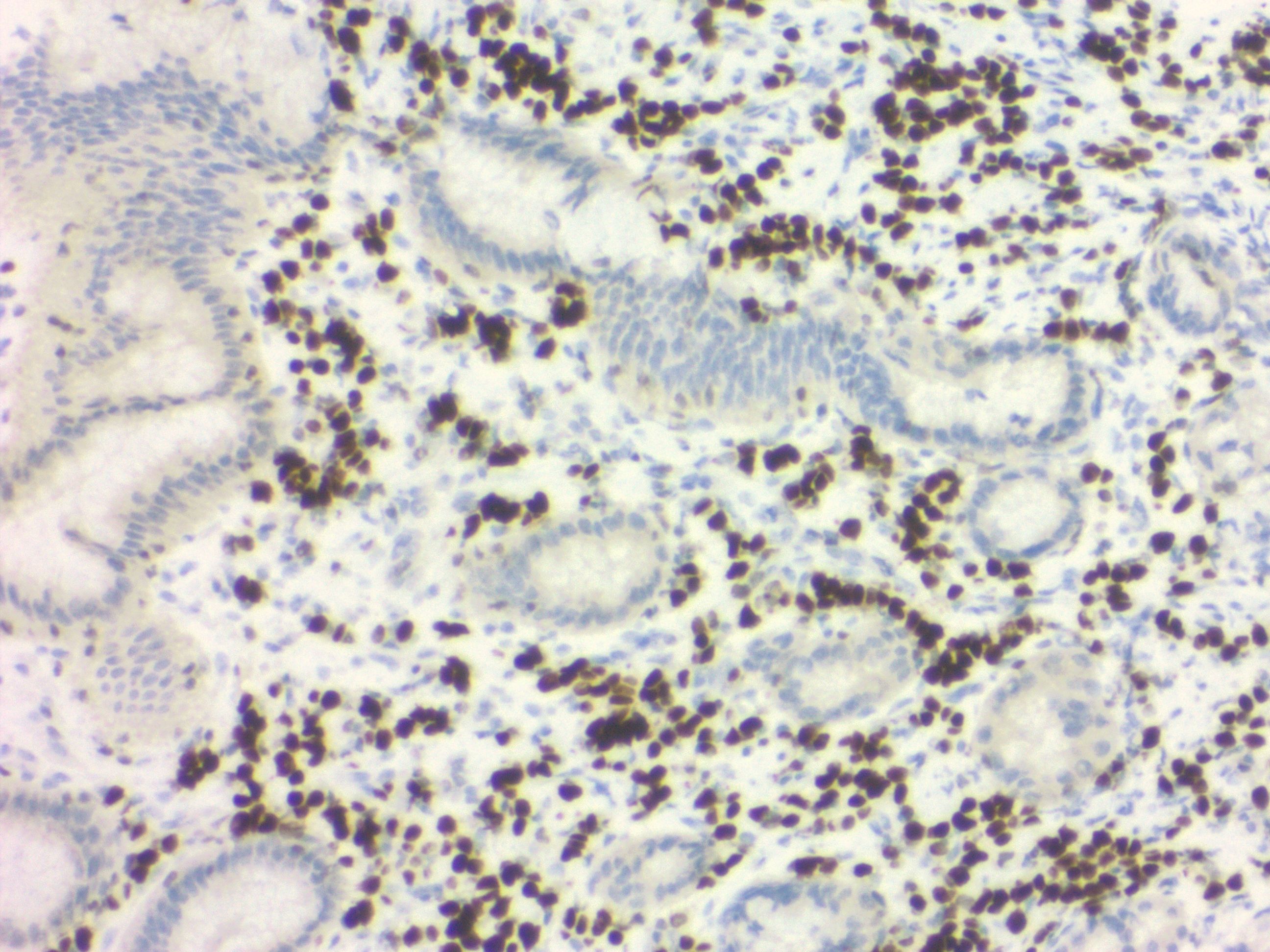
Methods: A 75-year-old female with a history of ILC in clinical remission since 2019 presented to our institution in fall 2024 with nausea, vomiting, decreased appetite, and a 10-pound unintentional weight loss. She was seen at a different hospital two months prior, where a CT of the abdomen showed mild thickening of the gastric wall, small bowel, terminal ileum, and cecum; infectious enterocolitis was suspected at that time. Due to persistent and worsening symptoms, we performed a repeat CT, which showed new moderate-volume ascites and persistent gastric wall thickening. We then performed an upper endoscopy, which revealed only mild erythema of the gastric mucosa, suggestive of possible gastritis. There was no mass, ulceration, or evidence of bleeding. However, random gastric biopsies showed infiltrating tumor cells in a linear arrangement in the lamina propria on H&E staining (Figure 1), which is typical of metastatic ILC. Immunohistochemistry was consistent with this and showed strong GATA3 positivity (Figure 2) and absence of CDX2, which is suggestive of metastatic and not primary gastric involvement.
Discussion: Identification of gastric involvement from metastatic breast cancer is challenging, as symptoms are nonspecific and endoscopic findings can be heterogeneous, with minimal or no obvious abnormalities in many cases. If gastric metastasis from breast cancer occurs, it is most likely due to ILC. A high index of suspicion is essential in patients with a history of ILC and unexplained GI symptoms. Obtaining histopathology and immunohistochemistry should be obtained when concern is sufficient, even if endoscopic findings are unremarkable.
Figure: Infiltrating invasive lobular carcinoma tumor cells in a linear arrangement in the lamina propria on H&E staining
Figure: Strongly positive GATA3+ staining, which is mainly seen in metastatic and not primary gastric cancer
Disclosures: Shiab Mussad indicated no relevant financial relationships. Jai Kumar indicated no relevant financial relationships. Serge Sorser indicated no relevant financial relationships.
Shiab Mussad, MD1, Jai Kumar, MD2, Serge Sorser, MD3. P4244 - Gastric Metastasis of Invasive Lobular Breast Cancer Presenting With Nonspecific GI Symptoms Five Years After Remission, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.