Gregory Riley, MD, Renee Williams, MD, MHPE, FACG, Carolyn Wilson, MD NYU Grossman School of Medicine, New York, NY Introduction: After an esophagectomy a gastric transposition, also known as a gastric pull up, is a procedure where the stomach is moved upwards into the chest and connected to the remaining healthy esophagus. This procedure restores the continuity of the GI tract to allow for swallowing and digestion of food. Literature to date reporting complications in gastric transposition is in children. Adult complications are not well elucidated. We illustrate a case of an adult patient, who developed an ulcer at the site of gastric transposition leading to a gastrobronchial fistula and subsequent aspiration.
Case Description/
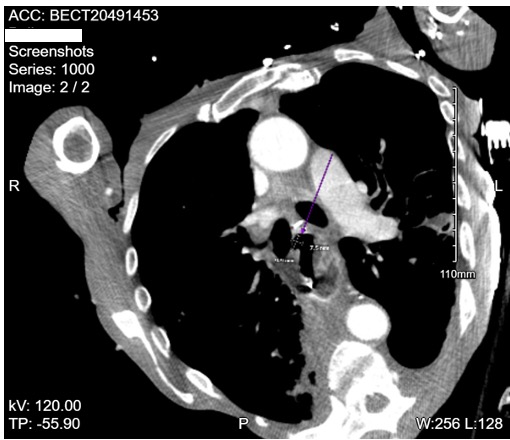
Methods: A 56-year-old male with a history of esophageal cancer s/p radiation therapy + esophagectomy w/ gastric transposition in 2002 presented from his clinic due to low oxygen saturation to 89%. Subjectively he reported 6 months of generalized weakness, decreased PO, weight loss, and frequent falls. Physical examination revealed a cachectic male with ecchymosis on the left chest wall and shoulder. CT chest was significant for multiple acute-subacute rib fractures on the left side and a large left sided empyema with internal gas locules which was thought to be secondary to bacterial seeding from the rib fractures. After drainage of the empyema and initial improvement, his course was complicated by severe acute hypoxemic respiratory failure requiring intubation. During mechanical ventilation it was noted he had an air leak on the ventilator. CT w/ IV contrast revealed a possible diverticulum in the conduit with proximity to the right mainstem bronchus (Figure 1). Bronchoscopy displayed air bubbles during expiration concerning for a tracheoesophageal fistula (figure 2, image A, B). A bedside EGD displayed a 20 mm ulcer in the gastric pull up, within the ulcer base was a small fistula opening consistent with a gastrobronchial fistula (Figure 2, image D). Additionally, a large amount of food residue was found within the pull up. Discussion: A gastrobronchial fistula is a rare complication post gastric pull up. Most described cases have been post Nissen fundoplication1 or post laparoscopic sleeve gastrectomy2. Post gastric transposition has only be described in pediatric cases, this is the first such case reported in an adult. Contrast study of the upper GI tract is widely used for diagnosis and one study found that 21 out of 25 reported cases were identified using contrast studies3. In our patient contrast study was negative possibly due to his severe kyphosis limiting his ability to lie supine.
Figure: Figure 1. A small diverticula approximates the right mainstem bronchus without definitive connection between the two structures.
Figure: Figure 2. Image A showing the airway normally. Image B showing the appearance of a bubble during expiration concerning for a gastrobronchic fistula. Image C is a recreation of the patients GI anatomy with labels of the biopsy portions. Image D taken from the stomach, EGD showing the bronchogastric fistula (upper right) and retained food contents.
Disclosures: Gregory Riley indicated no relevant financial relationships. Renee Williams indicated no relevant financial relationships. Carolyn Wilson indicated no relevant financial relationships.
Gregory Riley, MD, Renee Williams, MD, MHPE, FACG, Carolyn Wilson, MD. P4214 - A Rare Case of Gastrobronchial Fistula Presenting Post Gastric Transposition, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")