University of Alabama at Birmingham Huntsville, AL
Ross Hardin, DO, Aesha Patel, DO, John Fanning, MD, Addison Hardin, DO University of Alabama at Birmingham, Huntsville, AL Introduction: Emphysematous gastritis (EG) is a rare, severe form of gastritis characterized by intramural air in the gastric wall. While infection by gas-forming bacteria is the most common cause, rare cases of candida-induced EG has been documented.
Case Description/
Methods: A 71-year-old male with diabetes was admitted for acute hypoxic respiratory failure with tachycardia, tachypnea, elevated WBC count, and lactic acidosis concerning for sepsis. A CT angiogram showed scattered lung infiltrates and diffuse ground-glass opacities. Despite treatment with broad-spectrum antibiotics, steroids, and bronchodilators, his condition worsened, leading to ICU transfer for severe sepsis and respiratory distress resulting in intubation. A repeat CT revealed diffuse interstitial pneumonia and bronchoscopy showed thick, brown secretions with nondiagnostic bronchoalveolar cultures. Despite intervention, he developed multiorgan failure needing continuous renal replacement therapy. A positive T2 Candida panel led to micafungin treatment, but his condition deteriorated with rising lactic acid levels and abdominal distention. A CT scan of the abdomen showed a fluid-filled, distended stomach with air in the gastric wall, consistent with emphysematous gastritis. Surgical consults advocated for NG decompression and supportive care instead of surgery given his critical condition. Despite continued efforts, he did not improve and expired soon after compassionate extubation. Discussion: This case shows the complexities of EG, even in the setting of critically ill patients with sepsis and multiorgan dysfunction. The patient’s presumed lung infection initially guided treatment, but new signs—abdominal distention and worsening lactic acidosis—prompted consideration of an intraabdominal source, emphasizing the need to reevaluate sepsis etiology in deteriorating patients. An earlier GI consult could have expedited diagnosis by recognizing risk factors and aiding in endoscopic assessment. Lack of definitive treatment guidelines also makes EG challenging to manage. Surgical intervention was deferred in this case secondary to profound hemodynamic instability and poor prognosis, but has been proven to be effective in some cases. While early antifungal therapy, bowel rest, and NG decompression can lead to recovery without surgery, unfortunately for our patient, this was not the case. This shows the importance of early recognition, multidisciplinary involvement, and tailored management strategies when treating EG in candidemia.
Figure: Coronal CT of the abdomen allows for visualization of air present in the superolateral aspect of the gastric wall
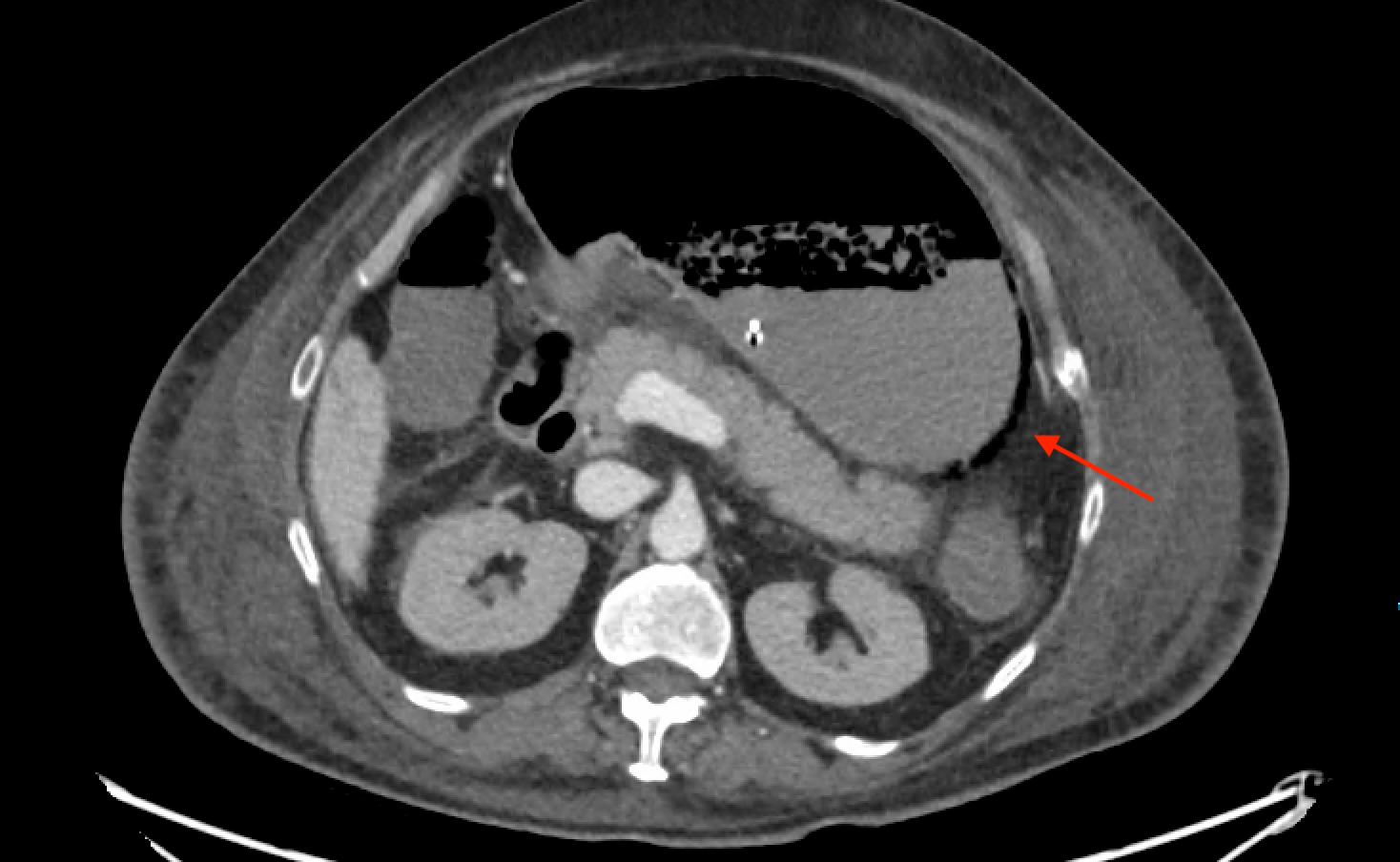
Figure: Gas can be visualized in the posterior aspect of the gastric wall (red arrow), consistent with emphysematous gastritis
Disclosures: Ross Hardin indicated no relevant financial relationships. Aesha Patel indicated no relevant financial relationships. John Fanning indicated no relevant financial relationships. Addison Hardin indicated no relevant financial relationships.
Ross Hardin, DO, Aesha Patel, DO, John Fanning, MD, Addison Hardin, DO. P4205 - An Unusual Case of Emphysematous Gastritis in the Setting of Candidemia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.