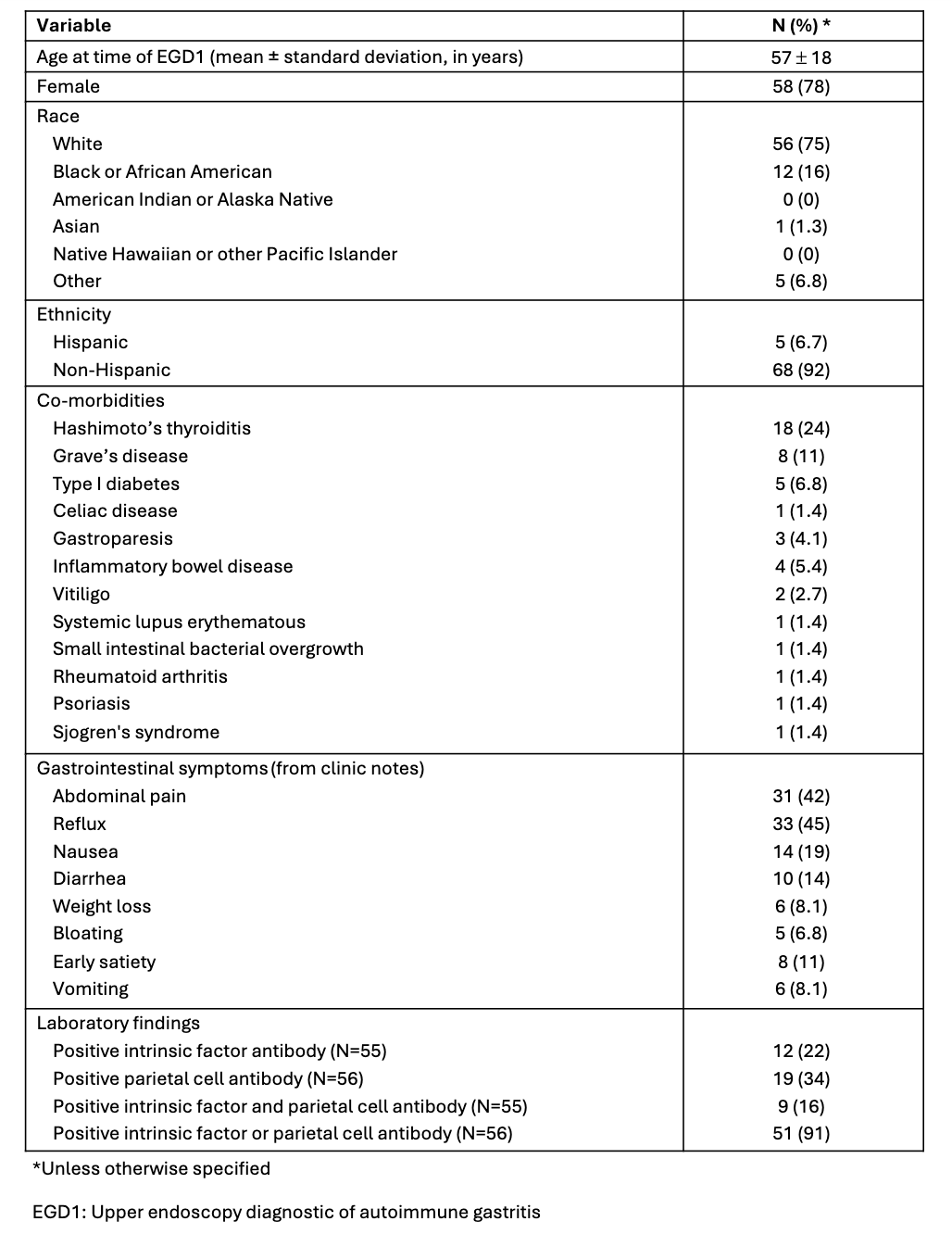
Joelle Bou Saba, MD1, Joseph Hajj, MD1, Joya-Rita Hindy, MD1, Tarek Souaid, MD, MPH1, John McMichael, PhD1, Kyungran Justina Cho, MD, PhD2, Michelle Kang Kim, MD, PhD3, Carol Rouphael, MD3 1Cleveland Clinic Foundation, Cleveland, OH; 2Cleveland Clinic Foundation, Pepper Pike, OH; 3Cleveland Clinic, Cleveland, OH Introduction: Autoimmune gastritis (AIG) is a chronic inflammatory disorder with progressive atrophy of the gastric oxyntic mucosa, which can progress to gastric intestinal metaplasia (GIM), dysplasia, and eventually gastric cancer (GC). AIG patients are also at risk for gastric neuroendocrine tumors (NET) type 1 due to gastrin up-regulation. Surveillance guidelines vary, recommending surveillance endoscopy (EGD) every 3-5 years or sooner in patients with NET or additional risk factors for GC. We assess the rate of pre-neoplastic and neoplastic lesions on follow-up EGD in AIG patients. Methods: In this retrospective cohort study, we included a random cohort of patients >18 with AIG diagnosed on index EGD (EGD1) between 2010 and 2022, and who had at least one follow-up EGD through 2025. AIG was defined by gastric biopsies showing corpus atrophy with enterochromaffin-like cell hyperplasia at EGD1. Exclusions were history of Helicobacter pylori infection, reflux esophagitis or gastrectomy. Pre-neoplastic lesions were defined as GIM or dysplasia, and neoplasia as NET or GC. Demographic and clinical characteristics were collected, as well as EGD and pathology characteristics at EGD1 and follow-up EGD with a new pre-neoplastic or neoplastic finding (EGD2). Descriptive statistics were used. A p-value < 0.05 was significant. Results: Of the 74 patients included, 78% were female and 75% White (Table 1). Mean age at EGD1 was 57±18 years and 91% of patients had positive AIG serologies. Patients had a mean of 3.0 ± 2.7 follow-up EGDs during the study period, and median time to first follow-up EGD was 1.5 [interquartile range (IQR), 3.4] years. At EGD1, 48 (65%) patients had GIM, 3 dysplasia, 9 NET and 1 gastric cancer (GC). At EGD2, 15 patients had new GIM, one had new low-grade dysplasia two years later, none had GC, and eight had new NETs. NETs were <10mm or found on random biopsies and only one was 15mm. Median time to EGD2 in patients with new NET was 2.1 (IQR, 4.2) years. Among the 51 patients with gastrin levels, those with NET at EGD1 or 2 (N=11) had higher mean gastrin compared to those without NET (N=40) (1658 ± 1217 vs 822 ± 866 pg/mL, p= 0.01). Discussion: Our findings emphasize need for endoscopic surveillance in patients with AIG. Surveillance intervals < 5 years may be warranted in patients with higher gastrin levels. Larger studies are needed to further determine optimal surveillance intervals for AIG patients and whether gastrin levels predict NET development.
Figure: Table 1: Demographic and clinical characteristics
Disclosures: Joelle Bou Saba indicated no relevant financial relationships. Joseph Hajj indicated no relevant financial relationships. Joya-Rita Hindy indicated no relevant financial relationships. Tarek Souaid indicated no relevant financial relationships. John McMichael indicated no relevant financial relationships. Kyungran Justina Cho indicated no relevant financial relationships. Michelle Kang Kim indicated no relevant financial relationships. Carol Rouphael indicated no relevant financial relationships.
Joelle Bou Saba, MD1, Joseph Hajj, MD1, Joya-Rita Hindy, MD1, Tarek Souaid, MD, MPH1, John McMichael, PhD1, Kyungran Justina Cho, MD, PhD2, Michelle Kang Kim, MD, PhD3, Carol Rouphael, MD3. P4196 - Pre-Neoplastic and Neoplastic Lesions at Follow-Up Endoscopy in Patients with Autoimmune Gastritis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Joelle Bou Saba, MD (she/her/hers) photo")