Udita Gupta, MD1, Nicholas Volpicelli, MD2, Michael Gavin, MD2 1University of New Mexico Hospital, Albuquerque, NM; 2New Mexico Veterans Affairs Hospital, Albuquerque, NM Introduction: Visceral artery pseudoaneurysms (VAPAs) are rare, most commonly involving splenic, renal, or hepatic arteries. Pseudoaneurysms are a recognized complication of both acute and chronic pancreatitis. Superior mesenteric artery (SMA) pseudoaneurysms are particularly uncommon. Duodenal hematomas in adults are typically associated with trauma, coagulopathy, or pancreatitis. However, they can rarely result from spontaneous hemorrhage of a visceral pseudoaneurysm. Here, we present an unusual case of gastric outlet obstruction (GOO) due to a duodenal hematoma secondary to a pseudoaneurysm of the SMA, in the absence of GI bleeding or trauma.
Case Description/
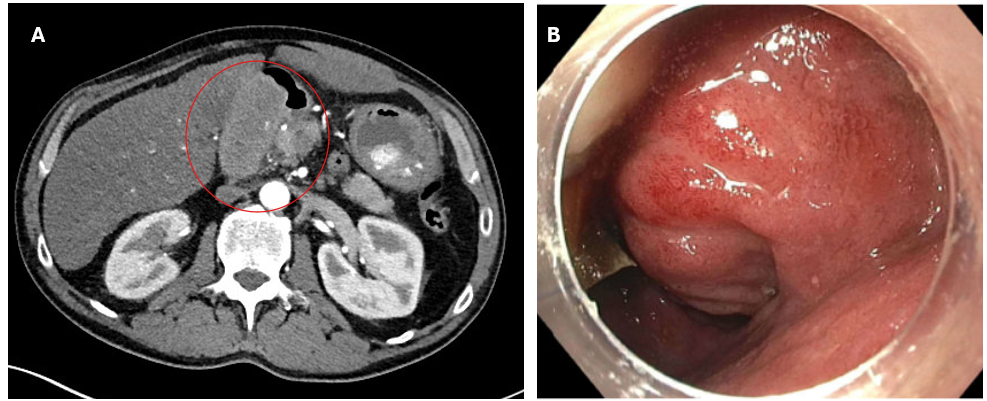
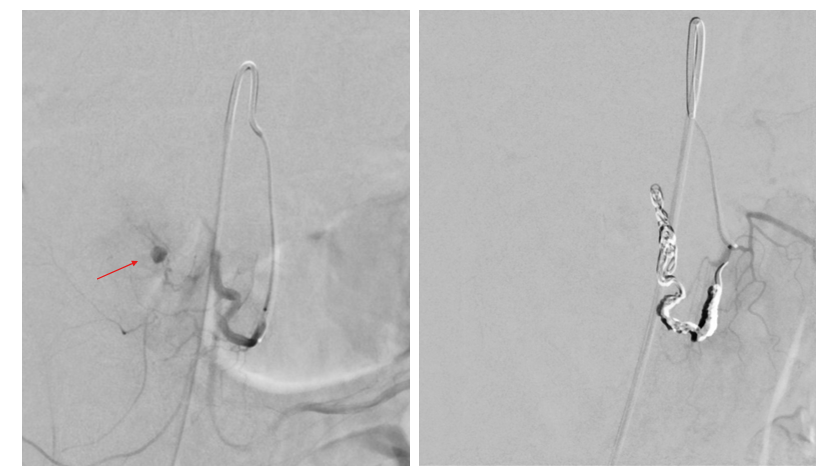
Methods: A 55-year-old male with history of alcohol-associated pancreatitis presented with 3 days of right-sided abdominal pain, nausea, vomiting, and inability to tolerate oral intake. He also reported a 10-pound weight loss over six months, recurrent nausea, and early satiety. There was no history of trauma. Examination revealed right upper quadrant tenderness. Hemoglobin was 13.2 g/dL, platelets 222 and INR 1.2. Abdominal CT showed heterogeneous density in the duodenum. (Fig 1A) MRI obtained for further characterization revealed a 7.2 × 3.3 × 5.1 cm well-encapsulated fluid collection suggestive of a hematoma. CT angiography showed active hemorrhage, though there were no clinical signs of GI bleeding. EGD showed retained gastric contents. After clearance, a large partially obstructive polypoid submucosal lesion with erythematous mucosa was seen in the duodenal bulb. (Fig 1B) Biopsies showed unremarkable mucosa. The second part of the duodenum and ampulla were normal. Given concerns for a vascular etiology, he underwent a mesenteric angiography with IR which identified a small pseudoaneurysm arising from an SMA branch. (Fig 2A) Multiple endovascular coils were deployed for successful embolization. (Fig 2B) The patient’s symptoms resolved post-procedure with improved oral intake. Discussion: This case is unique in both presentation and diagnosis, exemplifying a rare cause of GOO due to an SMA pseudoaneurysm. Pseudoaneurysm-related hemorrhage should be in the differential when submucosal duodenal lesions are encountered in association with hematomas, especially in patients with a history of pancreatitis. Early recognition of this rare but potentially life-threatening condition is essential, as a missed or delayed diagnosis may result in catastrophic hemorrhage.
Figure: Fig 1 A) CT showing abnormal density in duodenum suggestive of hematoma B) EGD with large submucosal duodenal bulb lesion
Figure: Fig 2: IR guided mesenteric angiography with A)superior mesenteric artery pseudoaneurysm B) post endovascular coil embolization
Disclosures: Udita Gupta indicated no relevant financial relationships. Nicholas Volpicelli indicated no relevant financial relationships. Michael Gavin indicated no relevant financial relationships.
Udita Gupta, MD1, Nicholas Volpicelli, MD2, Michael Gavin, MD2. P4148 - An Unusual Cause of Gastric Outlet Obstruction: Superior Mesenteric Artery Pseudoaneurysm, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.