Mansi Sheth, DO1, Sophia Pimpinelli, MD2, Anish V. Patel, MD2 1Jefferson Torresdale Hospital, Bridgewater, NJ; 2Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ Introduction: Lymphangiomas are malformations of the lymphatic system that are benign and uncommon. They can occur in the skin and mucous membranes. Small intestinal lymphangiomas are extremely rare. In this case, we present small intestinal lymphangiomas as an unlikely source of gastrointestinal (GI) bleeding.
Case Description/
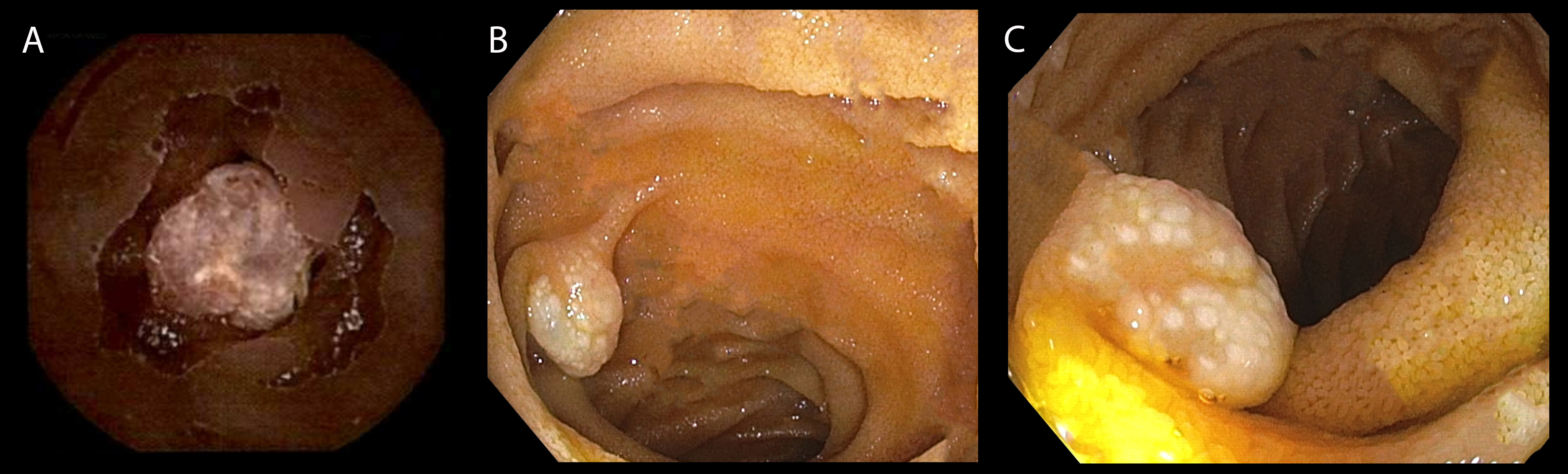
Methods: A 74-year-old Caucasian male with past medical history of chronic kidney disease with kidney transplantation (9 years ago), HIV (normal CD4 count), atrial fibrillation on Eliquis who presented to the emergency room for chest tightness and dyspnea. Cardiac evaluation found multi-vessel coronary occlusion and patient underwent triple vessel coronary artery bypass surgery (CABG). Six days later, he developed melena with acute blood loss anemia. Hemoglobin was noted to be 7.1g/dL from a baseline of 9.2-10.5 g/dL post CABG. Patient underwent esophagogastroduodenoscopy with no source of GI bleeding identified. Video capsule endoscopy was performed demonstrating several nodular polypoid lymphangiectasias scattered throughout the small bowel, of varying size. Large lesions in the jejunum were noted, one with ulceration (Figure 1A). To identify and characterize these lesions, push enteroscopy was performed. Nodular polypoid lymphangiectasias in the distal duodenum and proximal jejunum were identified (Figure 1B, C). One large lesion in the proximal jejunum was removed by mucosal resection for diagnosis. Pathology results demonstrated submucosal lymphangioma and no evidence of malignancy. After resection, patient was cleared to reinitate Eliquis with caution. Discussion: We present here a case of GI bleeding due to small bowel lymphangiomas. Lymphangiomas of the small intestine are very rare - those in the jejunum accounting for < 1% of all lymphangiomas. Majority is asymptomatic. Symptomatic patients have abdominal pain, GI bleeding, iron deficiency anemia, volvulus or bowel obstruction. Lymphangiomas are visualized as mucosal or submucosal masses on capsule endoscopy or enteroscopy. Treatment options typically include resection to prevent further bleeding, argon plasma coagulation for small bleeding focus, or small bowel resection if hemangioma is large and unable to be endoscopically resected. As a rare source of GI bleed, it is imperative for endoscopists to be aware of, identify and treat especially in those who require anticoagulation. Tissue diagnosis maybe important to rule out lymphoproliferative disorders especially in immunocompromised patients such as our patient.
Figure: Figure 1. A. lymphangioma visualized during video capsule with ulcerations. B. distal duodenum lymphangioma on endoscopy C. proximal jejunum lymphangioma on endoscopy.
Disclosures: Mansi Sheth indicated no relevant financial relationships. Sophia Pimpinelli indicated no relevant financial relationships. Anish Patel indicated no relevant financial relationships.
Mansi Sheth, DO1, Sophia Pimpinelli, MD2, Anish V. Patel, MD2. P4133 - Small Bowel Lymphangioma: An Unexpected Source of Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.