Anasua Deb, MD, PhD1, Grant Hutchins, MD2 1University of Nebraska Medical Center, Omaha, NE; 2Nebraska Medical Center, Omaha, NE Introduction: Diagnosis of metastatic small bowel melanoma can be challenging at times due to the often insidious nature of presentation and in many cases the anatomic location of the lesion. We describe a case of malignant melanoma with later metastasis to the small bowel that was originally suspected on video capsule endoscopy (VCE) and later confirmed histologically.
Case Description/
Methods: A 68-year-old female was referred to gastroenterology locally for severe fatigue and melena and was found to be profoundly anemic requiring urgent blood transfusion. Her PMH was notable for a malignant melanoma of the scapular region diagnosed nine years earlier. Initial management included excision and then treatment with adjuvant IFN which was ultimately discontinued due to cytopenia. Two years later she was found to have metastatic pulmonary nodules and was started on Pembrolizumab, which was later discontinued due to adrenal insufficiency, rash, and arthritis. She had remained off therapy with most recent CT/MRI 1 year prior without evidence of disease.
She presented to her local hospital due to profound fatigue and initial workup showed a Hgb of 6.4. She received 3 units of blood. Upper and lower endoscopies done for evaluation of anemia were non-revealing. A VCE was done revealing a lesion in the distal small intestine. A subsequent MRI enterography showed an ileal mass with polypoid component involved in the bowel wall. PET scan also confirmed an intensely avid metastatic lesion in the same location. A repeat colonoscopy with deep intubation of the terminal ileum was performed, with biopsy of the lesion confirming malignant melanoma. Surgical resection of the mass was successful. Discussion: Melanoma is the most common solid tumor metastasizing to the small bowel, with preference for jejunum and ileum. Diagnosis is often difficult as the symptoms are non-specific and the small intestine is not easily accessible with routine endoscopy. In our patient the presenting symptom was fatigue, and the initial endoscopic evaluation was normal. Ultimately the diagnosis of metastatic malignant melanoma to the small intestines was madethough VCE and a repeat colonoscopy. Our case shows that in the right clinical context, metastatic melanoma should be strongly considered. Additional diagnostic tests such as imaging studies, VCE and if needed double balloon enteroscopy should be considered in such patients to obtain definitive diagnosis.
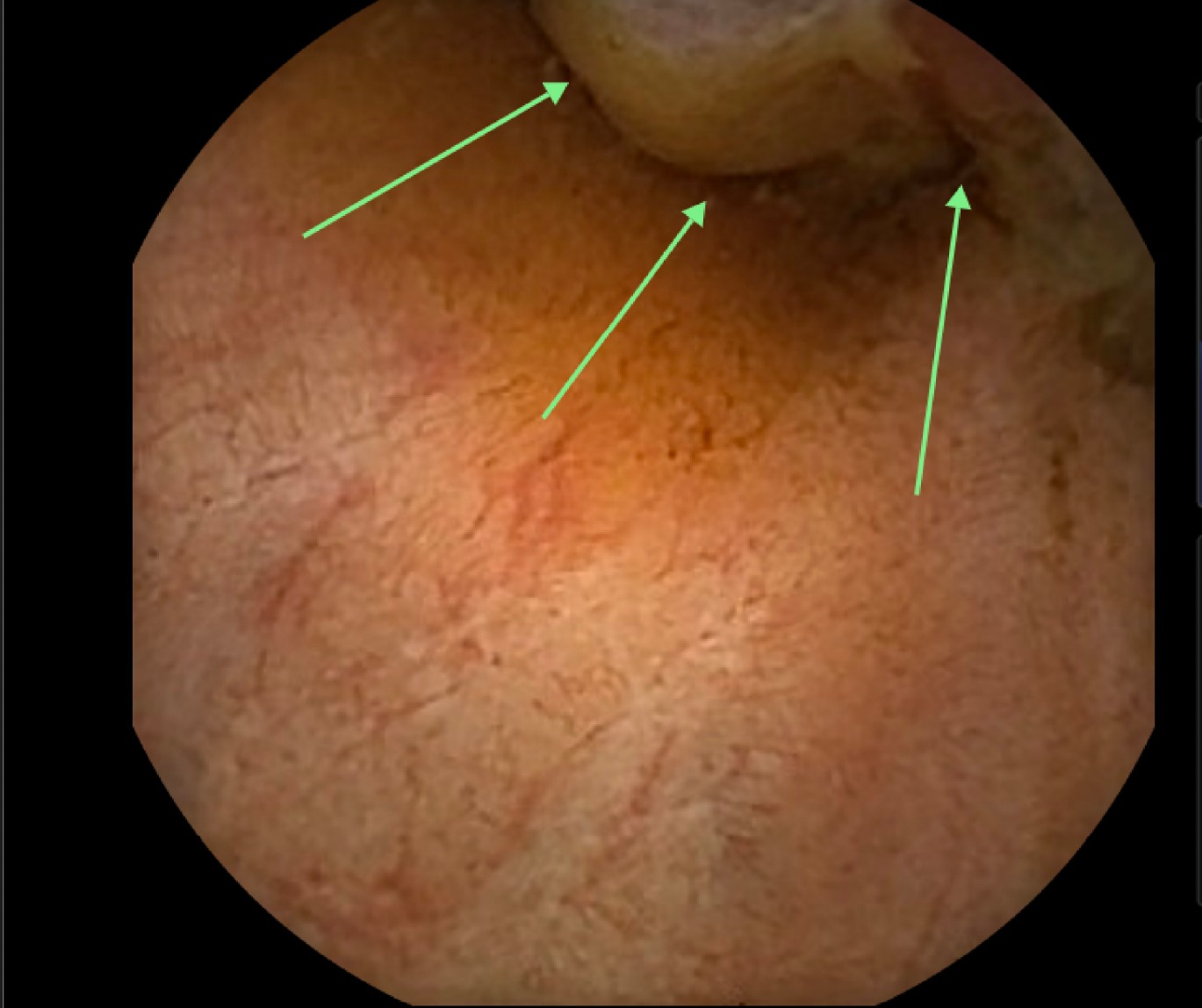
Figure: Video capsule endoscopy showing small bowel melanoma lesion
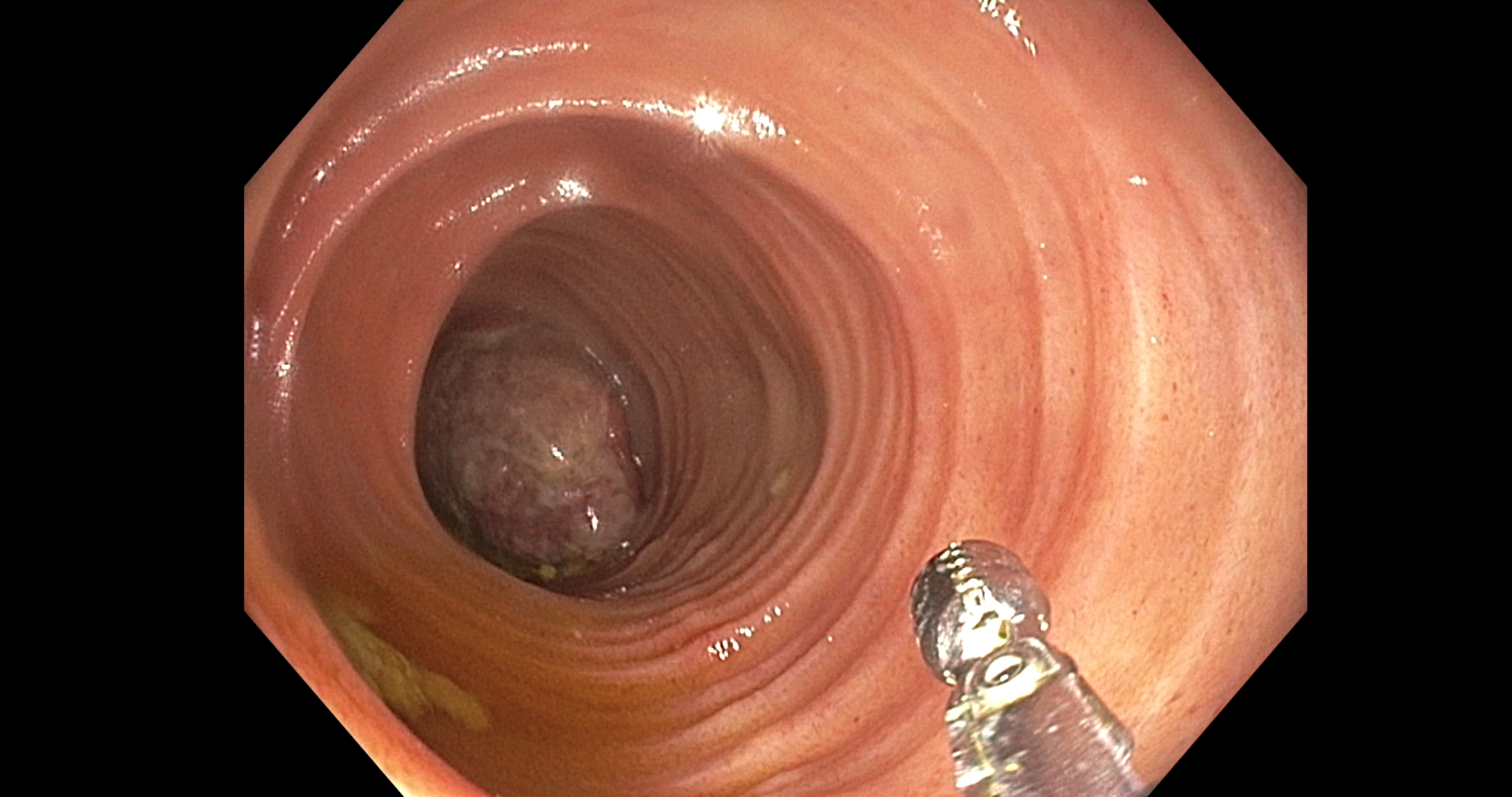
Figure: Colonoscopy with terminal ileum intubation showing small bowel mass
Disclosures: Anasua Deb indicated no relevant financial relationships. Grant Hutchins indicated no relevant financial relationships.
Anasua Deb, MD, PhD1, Grant Hutchins, MD2. P4130 - Metastatic Small Bowel Melanoma: A Diagnostic Challenge, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.