Ahmad Fouad Chaban, DO, Sameera Shuaibi, MD, Ian Tobal, DO Ochsner Health Clinic Foundation, New Orleans, LA Introduction: Müllerian duct adenocarcinoma, arising from tissues of the female genital tract, is a rare malignancy with an unusual pattern of metastasis to the gastrointestinal (GI) tract. While peritoneal seeding is the most common mode of spread, GI involvement is exceedingly rare. We present the case of a 70-year-old female with a history of stage IV serous ovarian adenocarcinoma in remission following surgical and medical therapy. After being lost to follow-up for several years, she presented with symptoms suggestive of an upper GI bleed and was ultimately found to have metastatic Müllerian disease involving the duodenum.
Case Description/
Methods: A 70-year-old female with stage IV serous ovarian carcinoma, previously treated with chemotherapy, BSO, peritoneal stripping, omentectomy, and resection of multiple abdominal masses in 2017, presented with several months of epigastric pain, weight loss, food aversion, and melena. She had been lost to follow-up since 2022, after discontinuing rucaparib. She denied NSAID, tobacco, or alcohol use and had no history of endoscopic evaluations.
In the ED, she was afebrile and hemodynamically stable. Labs revealed hemoglobin of 7.4 g/dL (baseline ~12) and MCV 73 fL. Exam showed conjunctival pallor and melena on rectal exam. She received IV pantoprazole and symptomatically improved, though her hemoglobin later dropped to 6.8 g/dL, requiring transfusion. CT imaging showed nodular thickening of the gastric antrum, pylorus, and duodenal bulb. EGD revealed LA Grade C esophagitis and an externally compressing duodenal mass, impeding scope passage. EUS confirmed a >5.5 cm hypoechoic, ulcerated mass in the proximal duodenal bulb with recent bleeding. Biopsies were consistent with recurrent Müllerian duct adenocarcinoma. Discussion: This case highlights a rare presentation of Müllerian duct adenocarcinoma metastasizing to the GI tract years after initial remission. Despite aggressive surgical debulking and peritoneal stripping, the patient developed late recurrence in the duodenum—an uncommon site for ovarian cancer spread. It emphasizes the importance of long-term surveillance and considering metastatic disease in patients with a remote cancer history presenting with new GI symptoms.
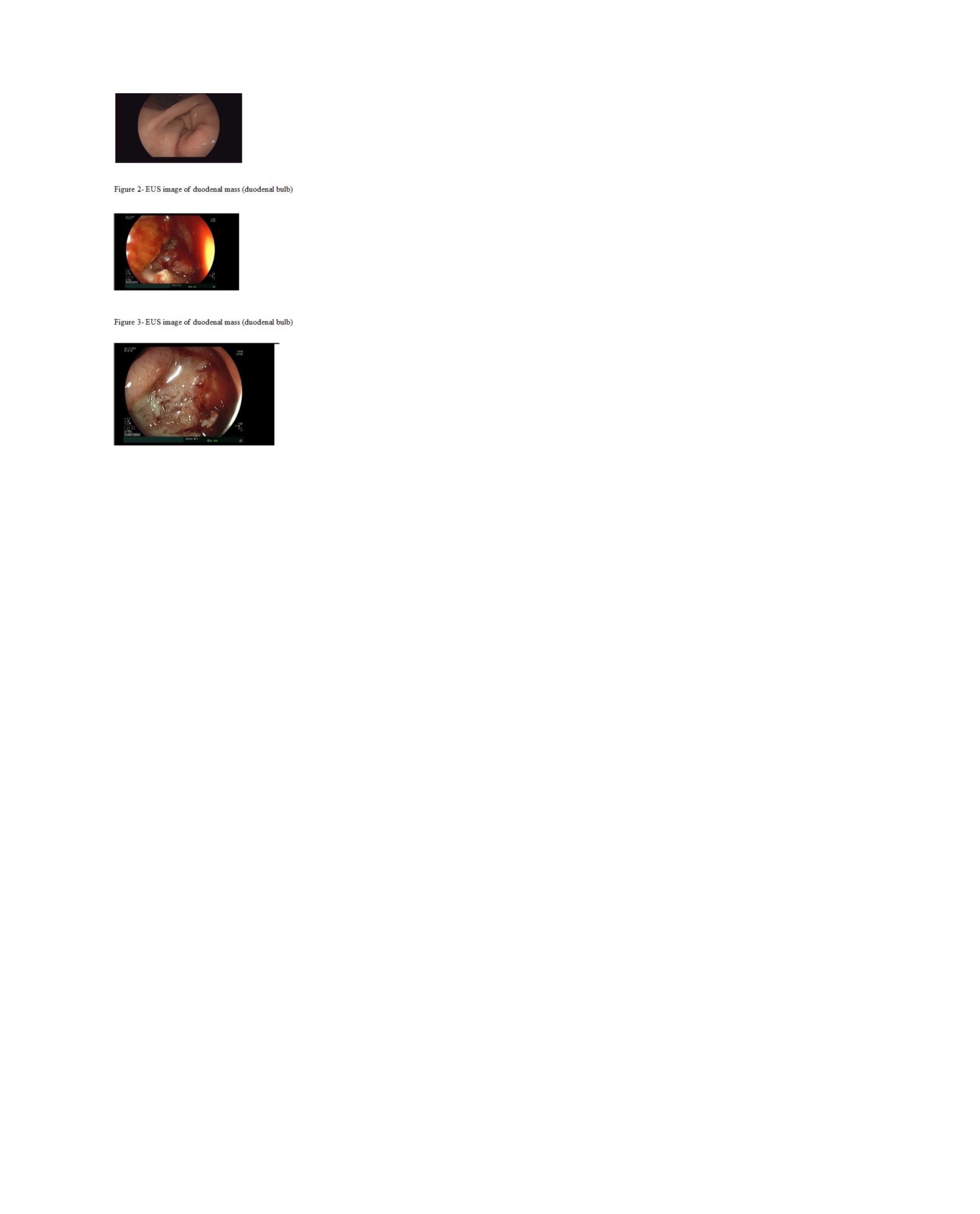
Figure: Figure 1- Gastric antrum- external compression leading to difficulty progressing EGD Figure 2- EUS image of duodenal mass (duodenal bulb) Figure 3- EUS image of duodenal mass (duodenal bulb
Disclosures: Ahmad Fouad Chaban indicated no relevant financial relationships. Sameera Shuaibi indicated no relevant financial relationships. Ian Tobal indicated no relevant financial relationships.
Ahmad Fouad Chaban, DO, Sameera Shuaibi, MD, Ian Tobal, DO. P4129 - Duodenal Ulcer Pathology: An Embryological Exploration, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")