Jessica Perry, MD1, Andrea Patete, DO2, Soundarapandian Baskar, MD3 1Methodist Le Bonheur Healthcare, Memphis, TN; 2Lincoln Memorial University - DeBusk College of Osteopathic Medicine, Harrogate, TN; 3AdventHealth, Tavares, FL Introduction: Small bowel tumors are rare, accounting for less than 5% of all gastrointestinal (GI) tract neoplasms, despite the small intestine comprising approximately 75% of the length and 90% of the mucosal surface area of the GI tract. Symptoms of small bowel tumors are typically nonspecific and lead to delayed diagnosis. Common diagnostic modalities include computed tomography (CT), magnetic resonance enterography (MRE), capsule endoscopy, and deep enteroscopy. This report presents a unique case of small bowel malignancy, contributing to the broader understanding of its clinical presentation, diagnostic considerations, and therapeutic challenges.
Case Description/
Methods: A 76-year-old man has a history of paroxysmal atrial fibrillation status post MAZE and watchman, coronary artery disease s/p CABG, hypertension, peripheral vascular disease, renal artery stenosis, chronic kidney disease, and small bowel AVM presented with a massive gastrointestinal (GI) bleed.Vital signs during admission demonstrated a temperature of 36.6°C, a heart rate of 71 beats/min, respirations of 15 breaths/min, and a blood pressure of 86/50 mmHg. On physical examination, the patient was alert, fully oriented, and in no acute distress. He had noticeable pallor and bruising on his skin. The complete blood count was remarkable for a white blood count of 15.08, hemoglobin of 8.7 with hematocrit of 27.1 and platelets were 287. The comprehensive metabolic panel was remarkable for bicarbonate 16, blood urea nitrogen 50, and creatinine of 1.90. Despite multiple esophagoduodenoscopies (EGDs) without clear evidence of GI hemorrhage and gastric artery embolization, the patient continued to have bleeding and anemia. A year after the initial presentation, push enteroscopy was performed with findings of proximal jejunum mass; biopsy proven jejunal adenocarcinoma. He underwent small bowel resection and adjuvant chemotherapy. Discussion: This is a distinctive case presentation of a small bowel tumor. Unfortunately for the patient presented here, there was a delay in diagnosis due to initial concerns of upper GI bleed. The ultimate source of the patient’s bleeding found a year after presentation was in the jejunum which is beyond the point expected to show signs of upper GI bleeding. There should be earlier consideration for video capsule endoscopy and/or enteroscopy in patients with refractory symptoms, unexplained anemia, or melena/GI bleed to help detect small bowel malignancies and reduce delays in diagnosis along with subsequent treatment.
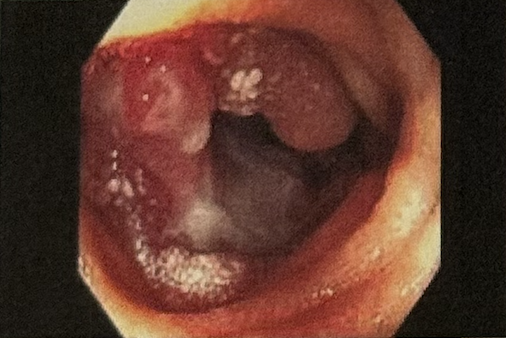
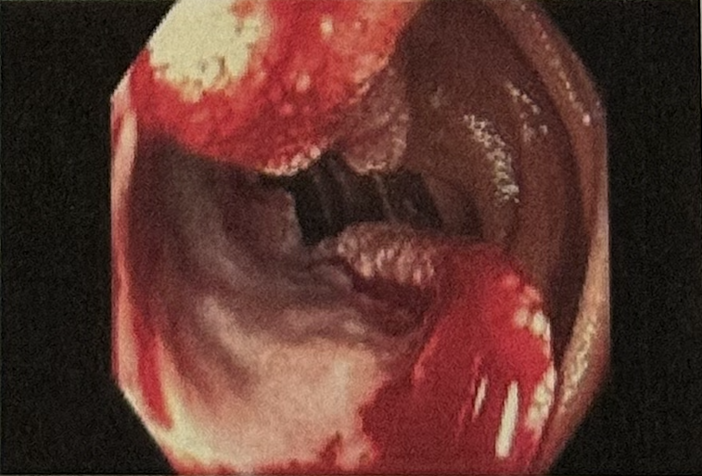
Figure: Proximal jejunum mass
Figure: Proximal jejunum mass
Disclosures: Jessica Perry indicated no relevant financial relationships. Andrea Patete indicated no relevant financial relationships. Soundarapandian Baskar indicated no relevant financial relationships.
Jessica Perry, MD1, Andrea Patete, DO2, Soundarapandian Baskar, MD3. P4127 - A Unique Case of a Small Bowel Tumor, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.