Department of Medicine, George Washington University School of Medicine and Health Sciences Washington, DC
Mrudula Bandaru, MD1, Zeina Bani Hani, MBBS1, Robert S.. Gordon, DO, MS2, Ankit Patel, MD3, Vinay Rao, MD4, Leen Raddaoui, MD4, Marie L. Borum, MD, EdD, MPH, FACG5 1Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC; 2George Washington University School of Medicine and Health Sciences, Arlington, WA; 3George Washington University School of Medicine and Health Sciences, Washington, DC; 4George Washington University Hospital, Washington, DC; 5Division of Gastroenterology and Liver Disease, Department of Medicine, George Washington University School of Medicine and Health Sciences, Washington, DC Introduction: Intestinal angina or chronic mesenteric ischemia (CMI) is caused by episodic intestinal hypoperfusion resulting in dull, crampy, postprandial pain. However, most individuals are asymptomatic due to an extensive collateral vascular network. Symptoms are more likely to occur in individuals >60 years of age, with dyslipidemia, atherosclerosis or tobacco use. Isolated duodenal ischemia has been rarely reported and can have up to a 40% mortality rate. We report a highly unusual case of isolated duodenal ischemia which was managed with angioplasty.
Case Description/
Methods: A 74-year-old male with hypertension, dyslipidemia, chronic kidney disease, 20-pack year smoking history, chronic back pain with NSAID use and recent gastrointestinal bleed presented with 1 week of melena, abdominal pain and fatigue. Exam revealed diffuse abdominal tenderness and melena on rectal exam. Labs were significant for hemoglobin of 11.5 g/dL and CT abdomen/pelvis showed possible enteritis and mild small-bowel ileus.
A push enteroscopy showed LA Grade D esophagitis without bleeding, pale gastric mucosa, non-bleeding ulcers in gastric antrum and duodenal bulb and diffuse severely friable mucosa with longitudinal ulcerations and areas of gangrenous tissue between the second and third portions of the duodenum consistent with intestinal ischemia. Biopsies of the area revealed small pieces of necrotic tissue with congestion and nonspecific reactive changes.
A CT angiogram uncovered extensive atherosclerotic disease with moderate stenosis of the proximal celiac artery and mild stenosis of the proximal superior mesenteric artery. The patient was treated with antibiotics, IV fluids and bedrest. Angioplasty of the proximal SMA resulted in improvement of the stenosis. There was no recurrent bleeding, thus he was discharged in stable condition. Discussion: CMI is a complex vascular disorder predominantly caused by the atherosclerotic occlusion of the mesenteric arteries, leading to postprandial pain and weight loss due to inadequate splanchnic blood supply or factors such as fear of eating. Due to its rarity and slow onset nature, it can be challenging to diagnose, requiring a high index of clinical suspicion. Revascularization is the definitive treatment for symptomatic CMI. Although surgery has been historically favored, endovascular interventions like percutaneous angioplasty and stenting have become the preferred initial approach due to lower perioperative morbidity and shorter hospital stays.
Figure: Esophagogastroduodenoscopy (EGD) capturing alternating longitudinal ulcerations with areas of black, gangrenous tissue extending from the second to the third portion of the duodenum.
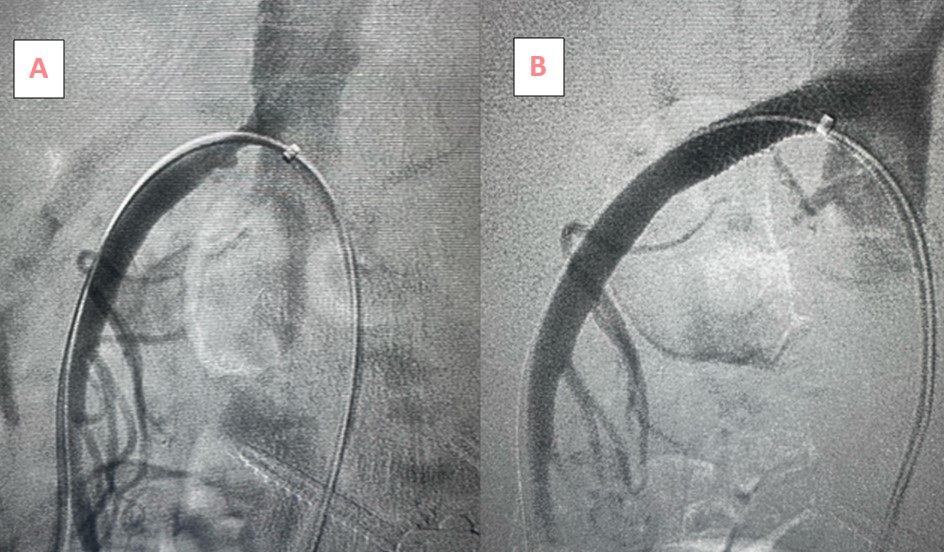
Figure: On CT angiogram, the proximal superior mesenteric artery was 50-60% stenosed (A) with significant improvement after bare metal stent employment (B).
Disclosures: Mrudula Bandaru indicated no relevant financial relationships. Zeina Bani Hani indicated no relevant financial relationships. Robert Gordon indicated no relevant financial relationships. Ankit Patel indicated no relevant financial relationships. Vinay Rao indicated no relevant financial relationships. Leen Raddaoui indicated no relevant financial relationships. Marie Borum indicated no relevant financial relationships.
Mrudula Bandaru, MD1, Zeina Bani Hani, MBBS1, Robert S.. Gordon, DO, MS2, Ankit Patel, MD3, Vinay Rao, MD4, Leen Raddaoui, MD4, Marie L. Borum, MD, EdD, MPH, FACG5. P4126 - Isolated Duodenal Ischemia: A Rare Case of Intestinal Angina, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")