Stacey Rolak, MD, MPH1, Mashal Batheja, MD2 1Mayo Clinic Arizona, Phoenix, AZ; 2Mayo Clinic, Scottsdale, AZ Introduction: There are multiple causes of mesenteric masses found on CT imaging for patients presenting with abdominal pain. We highlight a clinically significant case of sclerosing mesenteritis and the diagnostic approach to this condition.
Case Description/
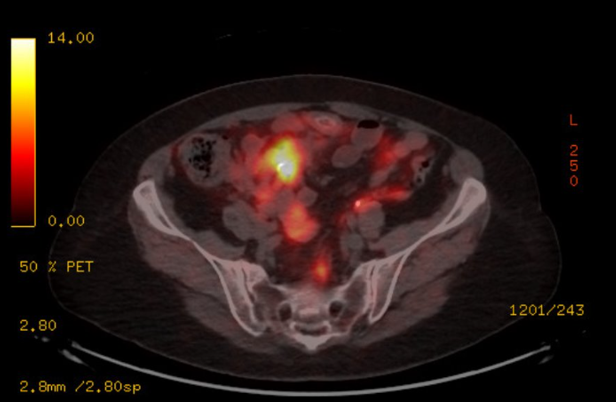
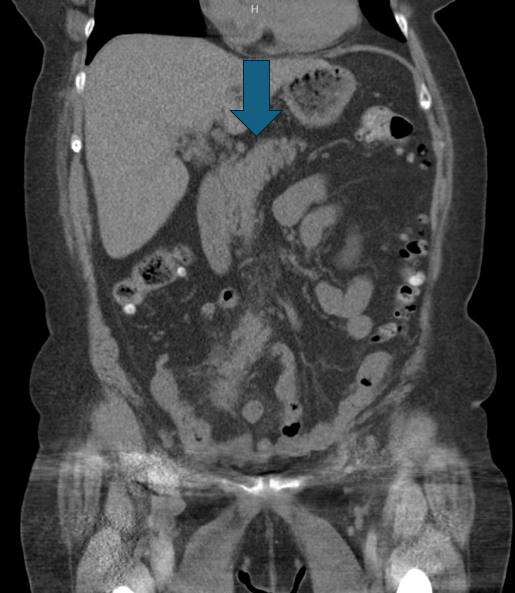
Methods: A 67-year-old female with a history of asthma presented for evaluation of 3 months of periumbilical abdominal pain worsening with oral intake, occasional nausea, and 15-pound weight loss. She had no previous abdominal surgeries. Vital signs were stable. There was no palpable mass on abdominal examination. Complete blood count, lipase, and comprehensive metabolic panel were unremarkable. Upper endoscopy with gastric biopsies and colonoscopy were unremarkable. CT abdomen/pelvis demonstrated a 2.6x3.8cm poorly encapsulated mesenteric mass with mesenteric stranding, no calcifications or tethering (Image 1). A DOTATATE PET scan revealed an ill-defined mesenteric mass with low grade somatostatin positivity and left axillary lymph node uptake (Image 2). Chromogranin A, plasma 5-HIAA, HIV testing, Coccidioides, tuberculosis, and connective tissue disorder testing were normal. Lymph node biopsy was unremarkable. She underwent an incisional biopsy of the mass with pathology showing extensive fat necrosis with chronic inflammatory changes. She was hospitalized for two partial small bowel obstructions with a transition point at the mass, which resolved with conservative management. Repeat CT imaging re-demonstrated the spiculated mass with central calcification. She underwent another biopsy of the mesenteric mass, with pathology again demonstrating fat necrosis, calcifications and chronic inflammation. Chromogranin, synaptophysin, Congo red staining, flow cytometry, and immunoglobulin testing on pathology were normal. She was initiated on treatment for sclerosing mesenteritis with prednisone and tamoxifen. At last follow-up she endorsed decreasing frequency of abdominal pain and had no recurrent hospitalizations. Discussion: Sclerosing mesenteritis is a non-neoplastic condition characterized by chronic fat necrosis, inflammation and fibrosis and should be considered in patients with abdominal pain presenting with a mesenteric mass on imaging. Lymphoma and metastatic neuroendocrine tumors should also be high on the differential, especially in those with weight loss and lymphadenopathy like in this patient. Biopsy and PET-CT may be needed if there is concern for malignancy. Steroids and tamoxifen are the mainstay of treatment.
Figure: CT abdomen/pelvis demonstrating 2.6 x 3.8cm mesenteric mass.
Figure: DOTATATE PET revealing an ill-defined mesenteric mass with low grade somatostatin positivity.
Disclosures: Stacey Rolak indicated no relevant financial relationships. Mashal Batheja indicated no relevant financial relationships.
Stacey Rolak, MD, MPH1, Mashal Batheja, MD2. P4124 - The Mystery of the Mesenteric Mass: A Case of Sclerosing Mesenteritis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.