James E. McSweeney, MD, Amrendra Mandal, MD South Georgia Medical Center, Valdosta, GA Introduction: NSAID-induced enteropathy is a lesser-known cause of terminal ileitis and strictures and can closely mimic Crohn’s disease in clinical presentation, imaging, and endoscopic findings. Differentiating between the two is essential to avoid unnecessary immunosuppression or surgical intervention.
Case Description/
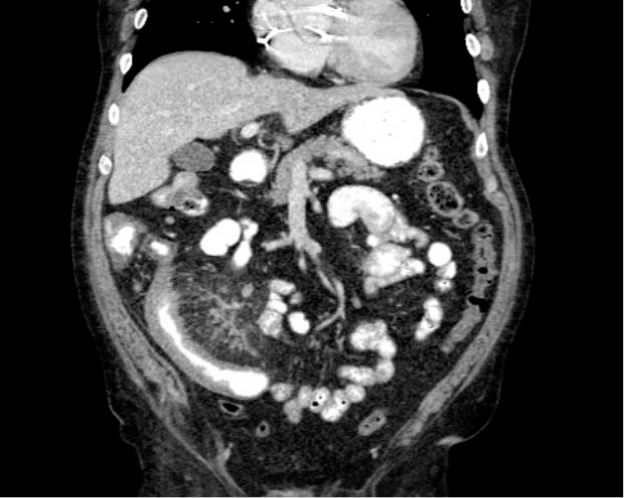
Methods: A 65-year-old male presented with epigastric pain, hematochezia, and unintentional weight loss. Contrast-enhanced CT abdomen revealed a markedly abnormal 16 cm segment of thickened terminal ileum with adjacent mesenteric fat stranding, prominent lymph nodes, and regional vascular engorgement (Fig1). These findings were strongly suggestive of active Crohn’s disease and led to a high index of suspicion for inflammatory bowel disease. Differential diagnoses included small bowel lymphoma or infectious ileitis; the elongated segment length made NSAID enteropathy less likely based on typical imaging patterns. Colonoscopy showed ulceration and a moderate stricture in the terminal ileum. Initial biopsies revealed only focal acute inflammation without chronic architectural distortion or granulomas. Fecal calprotectin levels were elevated (rising from 418 to 1080), reinforcing concern for active intestinal inflammation. However, repeat endoscopic biopsies again lacked features of chronic IBD. Following complete cessation of NSAIDs, the patient experienced significant clinical improvement, including 30-lb weight gain and resolution of gastrointestinal symptoms. Histologic re-review by a tertiary center supported NSAID-induced ileitis as the sole diagnosis. Discussion: This case underscores the diagnostic challenge posed by NSAID enteropathy when imaging mimics Crohn’s disease. The CT scan findings—long-segment terminal ileal thickening, mesenteric fat stranding, reactive lymphadenopathy, and vascular engorgement—are classic for active Crohn’s and atypical for NSAID injury, which is usually limited and less hyperemic. Elevated calprotectin further complicated the picture. Ultimately, the absence of histologic chronicity, full clinical remission after NSAID withdrawal, and specialist review helped establish the correct diagnosis. This case highlights the need for cautious interpretation of radiologic and biochemical data, and emphasizes the importance of longitudinal clinical correlation in patients with ileal disease.
Figure: Fig.1 Coronal section of CT abdomen/pelvis.
Disclosures: James McSweeney indicated no relevant financial relationships. Amrendra Mandal indicated no relevant financial relationships.
James E. McSweeney, MD, Amrendra Mandal, MD. P4111 - Terminal Ileal Stricture Due to NSAID Enteropathy Mimicking Crohn’s Disease: A Diagnostic Dilemma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.