Rebecca Moon, MD, MBA1, Allison Zemek, MD2, Elizabeth Dong, MD1, Marianne Fahmy, MD1 1Kaiser Permanente, Los Angeles, CA; 2Kaiser Permanente, Downey, CA Introduction: Immunoglobulin G4-related disease (IgG4-RD) is a fibroinflammatory, immune-mediated condition affecting various organs. Hepatopancreatobiliary involvement occurs in 30% of cases. Diagnosis is challenging due to nonspecific symptoms and lack of standardized criteria. Histology typically shows lymphoplasmacytic infiltration, storiform fibrosis, and elevated IgG4-positive plasma cells.
To date, only one case of small bowel IgG4-RD has been reported [1], presenting with bowel obstruction and recurrent strictures post-jejunal resection. Here, we report another rare case of small bowel IgG4-RD mimicking neoplastic or inflammatory disease.
Case Description/
Methods: A 75-year-old male with history of T-cell large granular lymphocytic (T-LGL) leukemia, pure red cell aplasia, and monoclonal gammopathy of undetermined significance (MGUS) presented with right lower abdominal pain, bloating and unintentional weight loss. Imaging showed circumferential thickening of the terminal ileum. Colonoscopy showed distorted ileal villi 10-15cm proximal to the ileocecal valve and biopsies revealed nonspecific lymphoid aggregates.
Due to concern for leukemic recurrence, he underwent laparoscopic ileocecal resection. Intraoperatively, thickened mesentery and narrowing of the ileum were noted. Surgical pathology showed dense lymphoplasmacytic infiltration and fibrosis. A thorough immunohistochemical work up was performed by Hematopathology which excluded involvement by lymphoma or leukemia. Persistent postoperative symptoms prompted additional staining of the pathology, which revealed increased IgG4-positive plasma cells (126/250 = 50.4% in a single high-power field). Serum IgG4 was elevated (116.2 mg/dL; normal < 86). He was diagnosed with IgG4-RD and treated with prednisone. One month later, symptoms improved, serum IgG4 normalized to 59.3 mg/dL, and imaging showed decreased small bowel enhancement. Discussion: Diagnosis was complicated by the patient's comorbidities as both T-LGL and MGUS can affect immunoglobulin levels and involve the GI tract, complicating interpretation of labs and imaging. Routine biopsy initially failed to identify IgG4-RD and diagnosis required targeted immunostaining.
Small bowel IgG4-RD is rare and can be challenging to differentiate from Crohn’s disease. Such misdiagnosis can potentially result in unnecessary surgery, as seen in this case. Awareness of this entity is critical to avoid misdiagnosis, guide appropriate therapy and prevent complications such as malnutrition and obstruction.
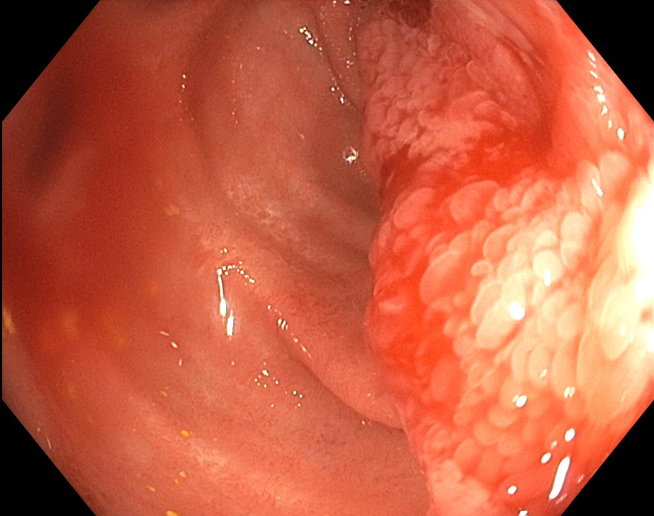
Figure: Terminal ileum with distorted villi
Figure: IgG4-positive plasma cells on pathology
Disclosures: Rebecca Moon indicated no relevant financial relationships. Allison Zemek indicated no relevant financial relationships. Elizabeth Dong indicated no relevant financial relationships. Marianne Fahmy indicated no relevant financial relationships.
Rebecca Moon, MD, MBA1, Allison Zemek, MD2, Elizabeth Dong, MD1, Marianne Fahmy, MD1. P4080 - Small Bowel Involvement of IgG4-Related Disease: A Diagnostic Challenge as a Crohn’s Disease Mimicker, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Rebecca Moon, MD, MBA photo")