Farah Issa, MD, Charles Uy, MD, John Kim, DO, Matthew Glover, MD Dignity Health St Rose Dominican, Las Vegas, NV Introduction: Rhabdomyolysis is defined as severe muscle injury, with subsequent release of its cellular constituents such myoglobin, electrolytes and proteins into circulation. Elevated liver enzymes are regularly observed in rhabdomyolysis, however acute liver failure is uncommon. Exact incidence is unknown due to sparse reports. We present a case of severe muscle injury/rhabdomyolysis causing acute liver failure.
Case Description/
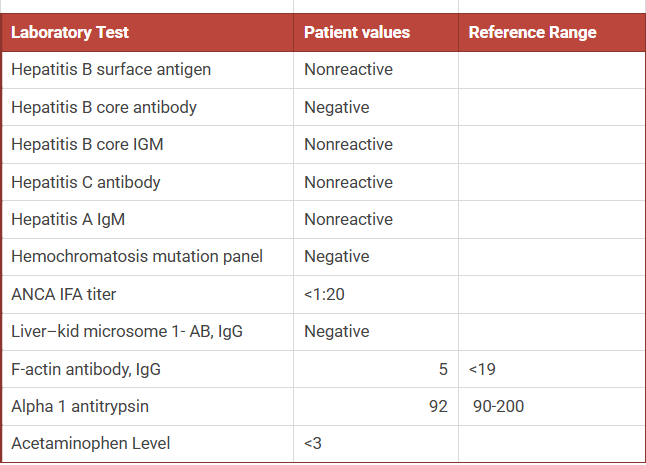
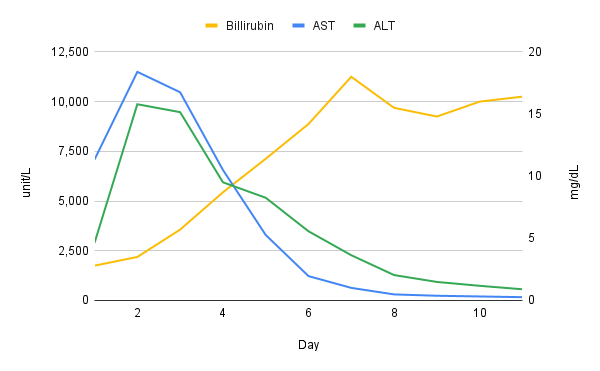
Methods: 63 year old male with past medical history significant for HTN, CKD stage 3a, renal cell carcinoma s/p left nephrectomy presented for sustained generalized weakness after a fall episode. The patient denied prior chronic liver disease. He denied supplement, herbal medicine or tylenol use. Initial vitals were within normal limits. Initial labs were notable for WBC 22.6 k/ul, hemoglobin 18 gm/dL, INR 2.24, creatinine 7.08 mg/dL, liver chemistry- bilirubin 2.8 mg/dL, ALT/AST 2,899/7,089 units/L, alkaline phosphatase 99 units/L and Creatine Kinase (CK) of 310,051 units/L. The patient was admitted to the hospital for management of severe rhabdomyolysis, acute liver failure and acute kidney failure. The patient subsequently developed hepatic encephalopathy, West-haven grade 2. Liver chemistry and INR continued to rise, peak INR- 7.4, peak ALT/AST- 9868/11,496 units/L, bilirubin peaked afterward at 18.0 mg/dL. Abdominal ultrasound doppler revealed patent hepatic vasculature. CT abdomen revealed unremarkable liver. Hepatic workup was largely negative, Figure 1. The patient was started on N-acetylcysteine empirically. Lactulose and rifaximin were initiated for his hepatic encephalopathy. He was treated with fluid resuscitation and started on hemodialysis for his concomitant kidney failure. Improvement of patient's rhabdomyolysis, resulted in parallel improvement of liver chemistry. Discussion: Although concomitant CK and liver chemistry elevations are frequently observed in rhabdomyolysis ( AST > ALT), acute liver failure secondary to rhabdomyolysis is exceedingly rare and sparsely reported. Underlying pathophysiology remains elusive, yet is postulated to be related to oxidative stress. Liver chemistry usually peaks within a few days and gradually declines along with improvement of rhabdomyolysis/muscle injury. Bilirubin is expected to lag in severe liver injury, as delta bilirubin forms; and takes longer to clear (half-life, 17-21 days). Hepatobiliary imaging is usually unremarkable. Unnecessary invasive tests such as liver biopsy should be avoided in such cases.
Figure: Figure 1: Hepatic workup
Figure: Figure 2: Liver Chemistry Trend
Disclosures: Farah Issa indicated no relevant financial relationships. Charles Uy indicated no relevant financial relationships. John Kim indicated no relevant financial relationships. Matthew Glover indicated no relevant financial relationships.
Farah Issa, MD, Charles Uy, MD, John Kim, DO, Matthew Glover, MD. P3987 - A Rare Case of Rhabdomyolysis-Induced Acute Liver Failure, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.