P3916 - Delayed FOLFOX-Associated Sinusoidal Obstruction Syndrome (SOS) in a Patient With Non-metastatic Stage IIC Colorectal Adenocarcinoma: A Case Report
Basil Jalamneh, MD1, Islam Mohamed, MD1, Moath Albliwi, MD1, Lana Dardari, MD2, Mohammed Janajri, MD3, Hamed Daw, MD1, Dakhil Noma, MD1 1Cleveland Clinic Foundation, Cleveland, OH; 2Cleveland Clinic Foundation, Westlake, OH; 3University of Central Florida, Gainesville, FL Introduction: Oxaliplatin is causally linked to the development and exacerbation of sinusoidal obstruction syndrome, which can precipitate or worsen portal hypertension. In this case, we report a delayed SOS secondary to oxaliplatin based chemotherapy in a patient with non-metastatic colorectal cancer.
Case Description/
Methods: A 48-year-old woman with stage IIC (T4bN0M0) colorectal adenocarcinoma underwent proctosigmoidectomy followed by 12 cycles of adjuvant FOLFOX. She had no hepatic metastases at diagnosis. After treatment, she reported weight gain, reflux symptoms, and joint pain. Surveillance imaging showed mild hepatic steatosis and borderline splenomegaly. One year later, labs showed mild transaminase elevation (AST: 37, ALT: 53) and normal bilirubin. Repeat CT scan showed new recanalization of the umbilical vein, raising concern for portal hypertension. MRI confirmed a recanalized paraumbilical vein without other signs of portal hypertension or metastasis. EGD was unremarkable except for mild gastritis. On EUS, the mean hepatic vein pressure was elevated (14mmHg), the mean portal vein pressure was mildly elevated (12 mmHg) and there was a normal portal-systemic pressure gradient (-2 mmHg). Eventually, liver biopsy showed centrilobular congestion, hepatocellular collapse and prominent portal veins suggestive of a vascular pattern of injury. Even though complete obliteration of central veins was not seen, findings were consistent with SOS due to the patient's clinical history and chemotherapy. Discussion: This case highlights the delayed onset of oxaliplatin-associated SOS in a patient without liver metastases. SOS typically presents with hepatomegaly, transaminase elevation, and features of portal hypertension, but radiologic and histologic findings may precede clinical signs. In this case, imaging revealed a spontaneous portosystemic shunt (SPSS) and sinusoidal changes prior to overt portal hypertension. The absence of portal systemic gradient elevation is mostly due to decompression through the SPSS. This case underscores the importance of long-term hepatic surveillance in CRC patients treated with oxaliplatin, even in the absence of metastatic disease. The absence of liver metastases in our patient suggests that direct oxaliplatin-induced endothelial toxicity was the primary driver of SOS, rather than tumor-related hepatic remodeling.
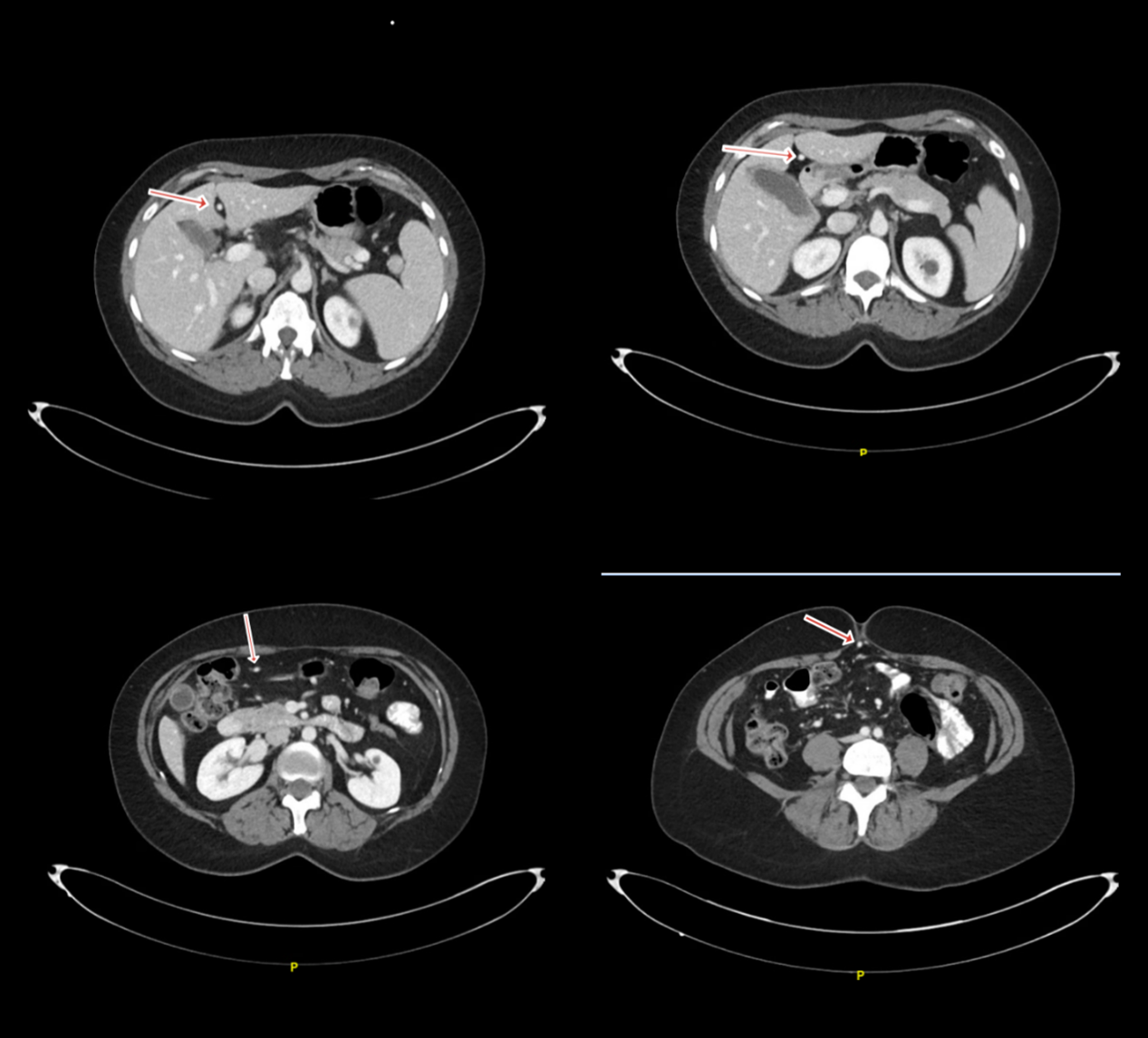
Figure: Image (1): recanalized umbilical vein (red arrow), running between 2nd, 3rd and 4th liver segments along the course of the falciform ligament. The recanalized vessel travels anteriorly and inferiorly toward the abdominal wall traversing through the umbilical fissure reaching the umbilicus.
Figure: Image (2): Coronal view showing recanalized umbilical vein running along the course of the falciform ligament.
Disclosures: Basil Jalamneh indicated no relevant financial relationships. Islam Mohamed indicated no relevant financial relationships. Moath Albliwi indicated no relevant financial relationships. Lana Dardari indicated no relevant financial relationships. Mohammed Janajri indicated no relevant financial relationships. Hamed Daw indicated no relevant financial relationships. Dakhil Noma indicated no relevant financial relationships.
Basil Jalamneh, MD1, Islam Mohamed, MD1, Moath Albliwi, MD1, Lana Dardari, MD2, Mohammed Janajri, MD3, Hamed Daw, MD1, Dakhil Noma, MD1. P3916 - Delayed FOLFOX-Associated Sinusoidal Obstruction Syndrome (SOS) in a Patient With Non-metastatic Stage IIC Colorectal Adenocarcinoma: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.