Prisma Health, University of South Carolina School of Medicine Columbia, SC
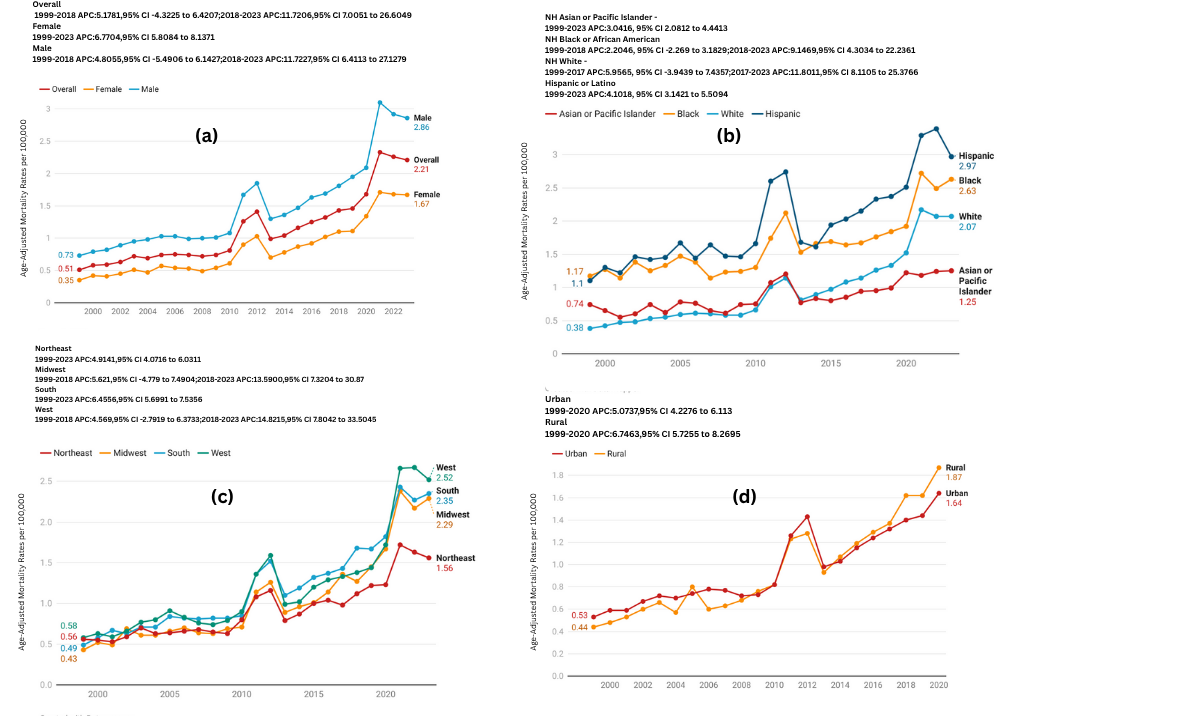
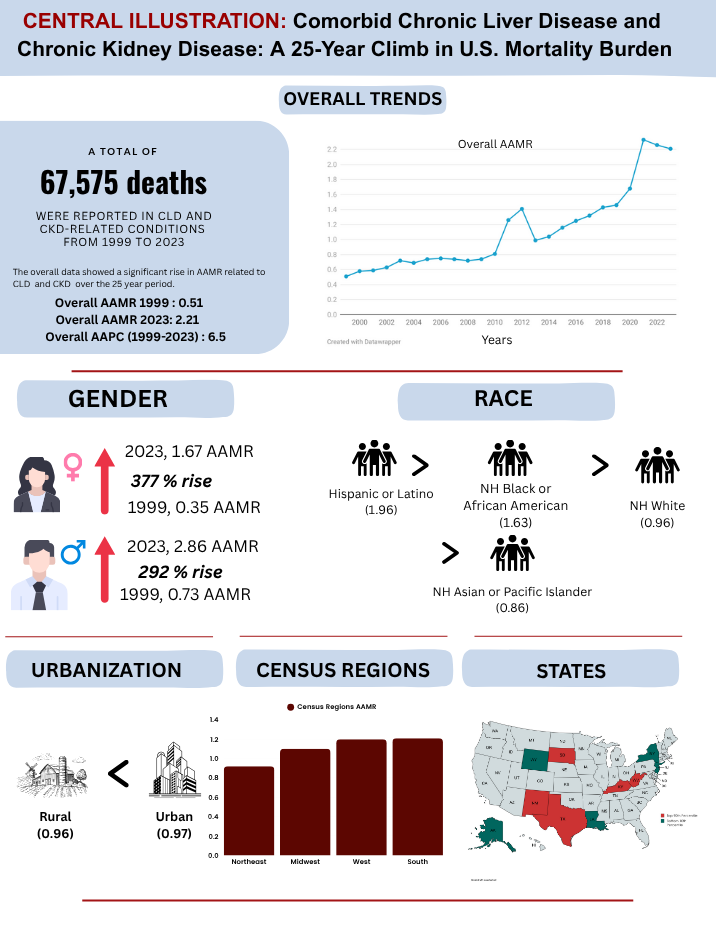
Susan Feldman, MD1, Simran Joshi, MD2, Muhammad Yamman bin irfan, MD3, Muhammad Khan, MD4, Muhammad Faizan Ali, MD5, Sherif Eltawansy, MD6, Saman Javaid, MBBS7, Noor ul Ain Saleem, 8 1Prisma Health, University of South Carolina School of Medicine, Columbia, SC; 2Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT; 3Shalamar Institute of Health Sciences, Lahore, Islamabad, Pakistan; 4Bacha Khan Medical College, Mardan, Islamabad, Pakistan; 5Jinnah Postgraduate Medical Centre, Karachi, Sindh, Pakistan; 6Jersey Shore University Medical Center, Jersey Shore, NJ; 7CMH Kharian, Sarghoda, Punjab, Pakistan; 8Fatima Memorial Hospital, Lahore, Punjab, Pakistan Introduction: Chronic liver disease (CLD) and chronic kidney disease (CKD) often coexist due to overlapping risk factors such as diabetes, hypertension, and alcohol use, resulting in increased morbidity and mortality. The interplay between these conditions exacerbates systemic inflammation and accelerates organ dysfunction, especially in aging populations. Despite this, national mortality trends and disparities associated with CLD and CKD have not been well characterized. This study examines trends in CLD and CKD-related mortality among U.S. adults from 1999 to 2023, focusing on demographic and geographic disparities. Methods: Mortality data from 1999–2023 were extracted from the CDC WONDER database using ICD-10 codes for CLD and CKD. Age-adjusted mortality rates (AAMRs) per 100,000 were calculated using the 2000 U.S. standard population. Joinpoint regression determined Annual Percent Change (APC) and Average Annual Percent Change (AAPC), with significance at p < 0.05. Analyses were stratified by sex, age group, race/ethnicity, U.S. census region, urbanization, and state. Results: There were 67, 575 CLD and CKD-related deaths, with 68.5% occurring in inpatient settings. AAMRs increased by 333% from 0.51 in 1999 to 2.21 in 2023 (AAPC: 6.5%, 95% CI: 4.7–7.8, p < 0.000001). Men had 49% higher mortality than women (1.42 vs. 0.95), but women experienced a slightly faster increase (AAPC: 6.8% vs. 6.2%). Mortality rose sharply with age: 0.12 (25–44), 1.14 (45–64), and 3.33 (65+), though the steepest growth occurred in ages 25–44 (AAPC: 7.3%). Hispanics had the highest AAMR (1.93), while non-Hispanic (NH) Asians had the lowest (0.83). NH Whites experienced a 445% increase in AAMR (0.38 to 2.07; AAPC: 7.4%). The South (1.31) and West (1.30) had the highest AAMRs, with the West showing the steepest rise (AAPC: 7.2%). Rural areas had slightly lower mortality than urban (0.94 vs. 1.02), but showed faster rise in mortality (AAPC: 6.7% vs. 5.1%). States in the top 90th percentile included South Dakota, West Virginia, New Mexico, Texas, and Kentucky. Discussion: From 1999 to 2023, mortality from comorbid CLD and CKD rose 333%, with the highest burden in older adults, men, Hispanics, and residents of the South and West. Notably, the steepest increase was seen in young adults (25–44 years) and rural populations, underscoring the need for early detection and targeted public health strategies.
Figure: Age-adjusted mortality Rates per 100,000 over time
Figure: pictorial
Disclosures: Susan Feldman indicated no relevant financial relationships. Simran Joshi indicated no relevant financial relationships. Muhammad Yamman bin irfan indicated no relevant financial relationships. Muhammad Khan indicated no relevant financial relationships. Muhammad Faizan Ali indicated no relevant financial relationships. Sherif Eltawansy indicated no relevant financial relationships. Saman Javaid indicated no relevant financial relationships. Noor ul Ain Saleem indicated no relevant financial relationships.
Susan Feldman, MD1, Simran Joshi, MD2, Muhammad Yamman bin irfan, MD3, Muhammad Khan, MD4, Muhammad Faizan Ali, MD5, Sherif Eltawansy, MD6, Saman Javaid, MBBS7, Noor ul Ain Saleem, 8. P3803 - Comorbid Chronic Liver Disease and Chronic Kidney Disease: A 25-Year Climb in US Mortality Burden, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")