Eugene Park, MD, Sophia Bostwick, DO, Jeremy Lake, MD, Nada Mohamed, MD Oregon Health & Science University, Hillsboro, OR Introduction: Acute on chronic pancreatitis can lead to surrounding tissue inflammation, forming a walled-off fluid collection, or a “pseudocyst”. Common complications of a pancreatic pseudocysts include infection or, rarely, fistulization to nearby structures. Usual areas of fistulization include the stomach, duodenum, and colon. Here, we present a case of pancreatitis complicated by a pancreatic pseudocyst with fistulization into the mediastinum.
Case Description/
Methods: A 49-year-old female with chronic alcohol use initially presented with dyspnea, and was found to have necrotizing pancreatitis and peripancreatic fluid collections with bilateral pleural effusions. Over the next year, she had several admissions for ongoing dyspnea and abdominal pain, complicated by loculated pleural effusions and definitive pancreatic pseudocyst formation. A magnetic resonance cholangiopancreatography (MRCP) showed extension of the pancreatic pseudocyst into the mediastinum. Repeat imaging months later showed persistence of the mediastinal pseudocyst with tracking into the esophageal hiatus. An endoscopic retrograde cholangiopancreatography (ERCP) was completed for placement of biliary and pancreatic duct stents. Due to persistent symptoms, a repeat ERCP was performed, resulting in pancreatic duct dilation and placement of a second bile duct stent. The patient clinically improved and remained sober from alcohol, with complete resolution of the mediastinal pseudocyst. Discussion: As fistulization of pancreatic pseudocysts into the mediastinum are rare, management is challenging as there are few cases documented. Management is focused on drainage and limiting pancreatic fluid spread. Control of pancreatitis is key, as demonstrated by our case, as a combination of both surgical intervention and alcohol cessation led to a favorable outcome.
Figure: Initial MRCP demonstrating new 2.0 cm posterior mediastinal pseudocyst extending from pancreatic pseudocyst
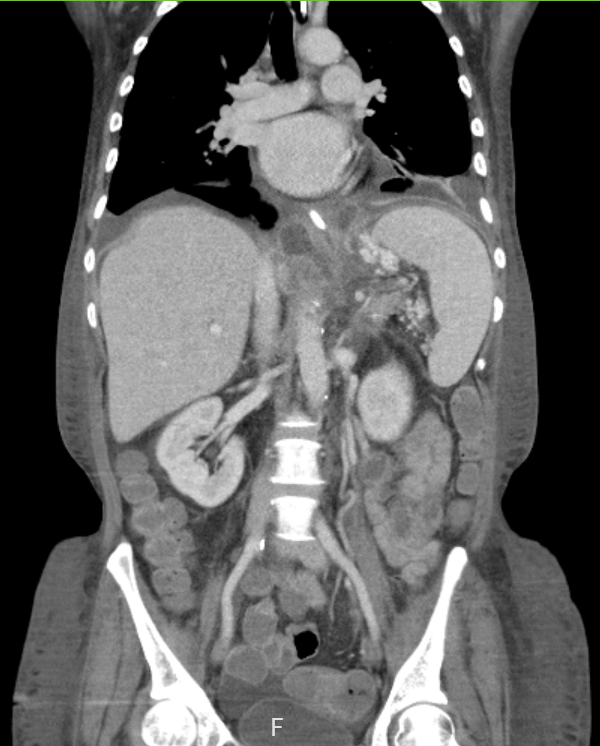
Figure: 8 month follow up CT chest, abdomen, and pelvis post pancreatic stent placement with interval improvement in mediastinal pseudocyst size
Disclosures: Eugene Park indicated no relevant financial relationships. Sophia Bostwick indicated no relevant financial relationships. Jeremy Lake indicated no relevant financial relationships. Nada Mohamed indicated no relevant financial relationships.
Eugene Park, MD, Sophia Bostwick, DO, Jeremy Lake, MD, Nada Mohamed, MD. P4426 - A Case of Necrotizing Pancreatitis Complicated by Pancreatic Pseudocyst With Mediastinal Fistulization, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.