McKenna Andrews, MD1, David W. Berry, DO2, Aamir-Ali Shaikh, BS, MPH3, Hezborn Magacha, MD2, Venkata Pulivarthi, MD2 1East Tennessee State University, Kingsport, TN; 2East Tennessee State University, Johnson City, TN; 3East Tennessee State University, Knoxville, TN Introduction: Hyperkinetic gallbladder syndrome is an underrecognized cause of right upper quadrant (RUQ) abdominal pain, characterized by elevated gallbladder ejection fraction (GBEF >80%) on hepatobiliary iminodiacetic acid (HIDA) scan in the absence of gallstones. The pathophysiology is thought to involve increased sensitivity to cholecystokinin (CCK), leading to excessive gallbladder contractility. Glucagon-like peptide-1 (GLP-1) receptor agonists, such as tirzepatide, are known to inhibit gallbladder emptying and reduce CCK release. However, the implications of discontinuing these agents on gallbladder motility are poorly understood.
Case Description/
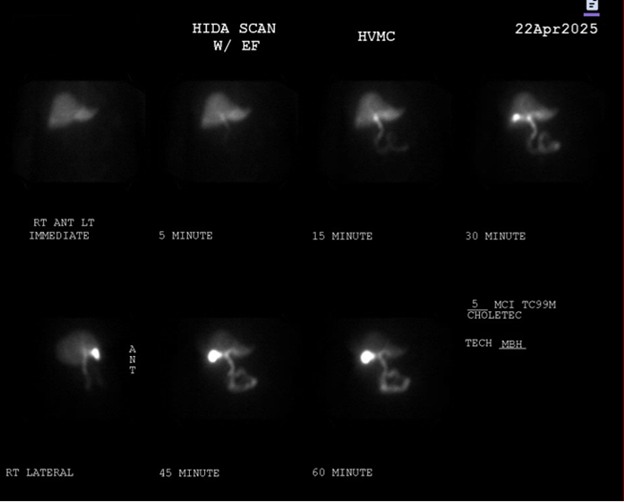
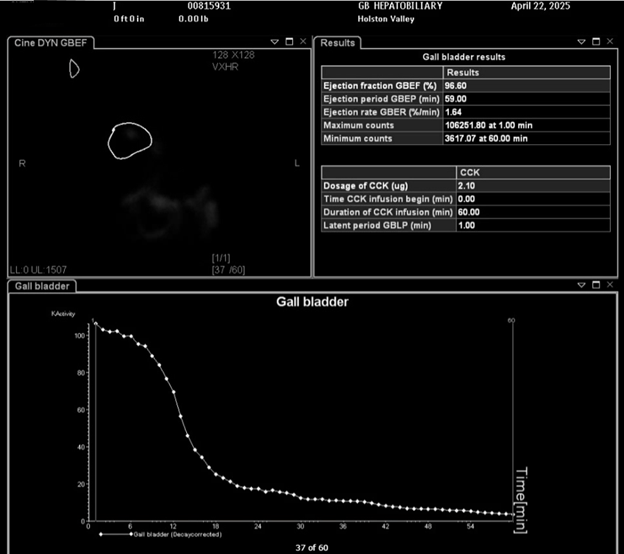
Methods: A 71-year-old female with a history of type 2 diabetes mellitus (T2DM), gastroesophageal reflux disease (GERD), and recent use of the GLP-1 receptor agonist tirzepatide presented with several months of intermittent, postprandial RUQ pain. Symptoms began approximately 2–3 months after she discontinued tirzepatide, which she had used for six months. The patient was unable to continue tirzepatide therapy due to financial constraints. Laboratory testing including liver enzymes and bilirubin was normal, though lipase was mildly elevated. Abdominal ultrasound was unremarkable without evidence of gallstones or biliary duct dilation. Esophagogastroduodenoscopy (EGD) showed mild esophagitis but no ulcers or strictures. A HIDA scan with CCK stimulation revealed a GBEF of 94.9%, consistent with hyperkinetic biliary dyskinesia (Images 1 and 2). After consultation with surgery, the patient underwent laparoscopic cholecystectomy. Pathology revealed a normal gallbladder. At follow-up, she reported complete resolution of abdominal pain. Discussion: This case underscores hyperkinetic gallbladder as a potential cause of RUQ pain, especially in patients with a normal ultrasound and no evidence of cholelithiasis. While GLP-1 receptor agonists are known to inhibit gallbladder motility, this case suggests that discontinuation may lead to a rebound hypercontractile state due to restored or hypersensitized CCK pathways. To our knowledge, this is among the first reported cases of hyperkinetic biliary dyskinesia temporally associated with cessation of GLP-1 therapy. HIDA scan with CCK stimulation is a valuable diagnostic tool when standard imaging is non-revealing. Cholecystectomy remains the definitive treatment, with favorable outcomes reported in symptomatic patients with elevated GBEF.
Figure: Image 1. HIDA scan showing hyperkinetic activity of the gallbladder.