Osama Abdur Rehman, MD, Iryna S. Hepburn, MD, FACG Florida State University, Cape Coral, FL Introduction: Biliary strictures are often concerning for malignancy, but benign infection or inflammation may also contribute to their formation. Distinguishing between the two is critical, as management and prognosis vary. We present a patient with biliary obstruction from multiple strictures due to a duodenal ulcer.
Case Description/
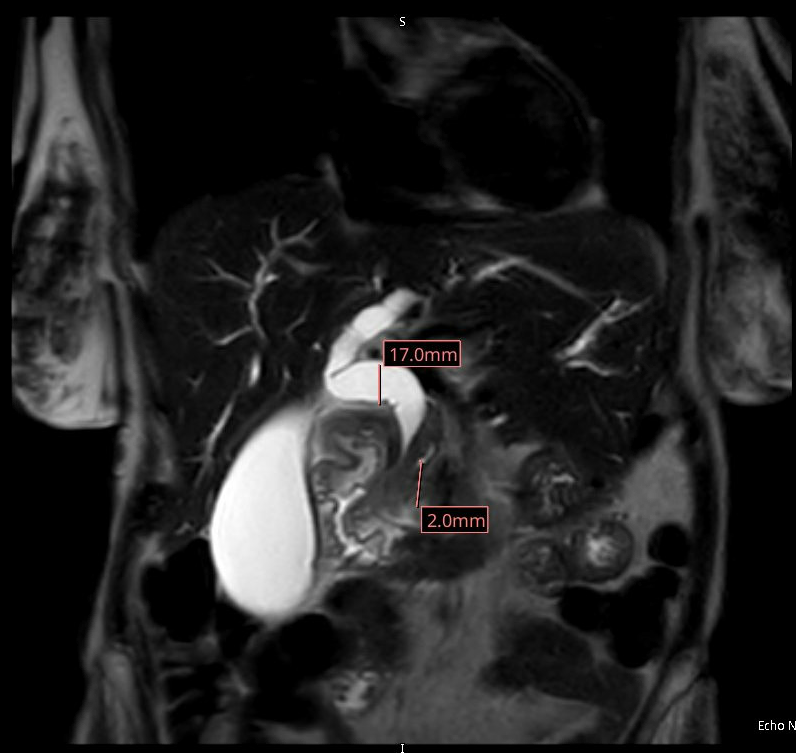
Methods: A 70 y/o female came to ED with RUQ abdominal pain. Laboratory data showed Hg 6.8 g/dL, alk phos 353 U/L, AST106 U/L, ALT 186 U/L, Tbili 4.7. CT noted intra- &extrahepatic biliary dilation and distended gallbladder, but no gallstones. MRCP showed strictured CBD at the level of the pancreatic head, and short stricture of the proximal CHD, but no features of cholecystitis or mass. ERCP was planned for presumed malignancy. Endoscopic evaluation revealed a deep duodenal ulcer occupying ¾ of the first and second portions of the duodenum including the area of papilla. H. pylori testing was negative. No endoscopic features of malignancy were noted and the biopsies were negative. Given the ampullary involvement in the ulcer, the strictures were attributed to inflammation.The patient was given high-dose PPI therapy. Liver enzymes gradually improved. At the time of discharge, LFTs had nearly normalized. On follow-up EGD and MRCP, both the ulcers and strictures were noted to have resolved. Discussion: Benign biliary strictures due to ulcer disease are a rare cause of biliary obstruction and mostly involve distal CBD. Stricturing of the CHD due to ulcer is even more rare. While malignant etiologies are often prioritized in the differential, the absence of a pancreatic mass, presence of a duodenal ulcer encroaching on the ampulla, and resolution of biliary obstruction with PPI supports the diagnosis of a benign process in this case. Duodenal ulcers can lead to biliary obstruction via local inflammation, edema, or fibrosis, particularly when involving the second part of the duodenum. Inflammatory strictures typically appear smooth and tapered on imaging, unlike the irregular or nodular margins seen in malignancy.This case highlighted the fact that medical management with PPI therapy can lead to resolution of both ulcer and biliary abnormalities which helped to avoid invasive procedures. In patients presenting with biliary obstruction and duodenal ulcer in the periampullary region, benign inflammatory strictures should be considered. After establishing the correct diagnoses with radiographic and endoscopic modalities, simple medical therapy and close monitoring might be sufficient.
Figure: Dilated CBD ending in a stricture
Disclosures: Osama Abdur Rehman indicated no relevant financial relationships. Iryna Hepburn indicated no relevant financial relationships.
Osama Abdur Rehman, MD, Iryna S. Hepburn, MD, FACG. P4488 - When Ulcers Obstruct: Unmasking Large Duodenal Ulcer as a Hidden Cause of Obstructive Jaundice, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")