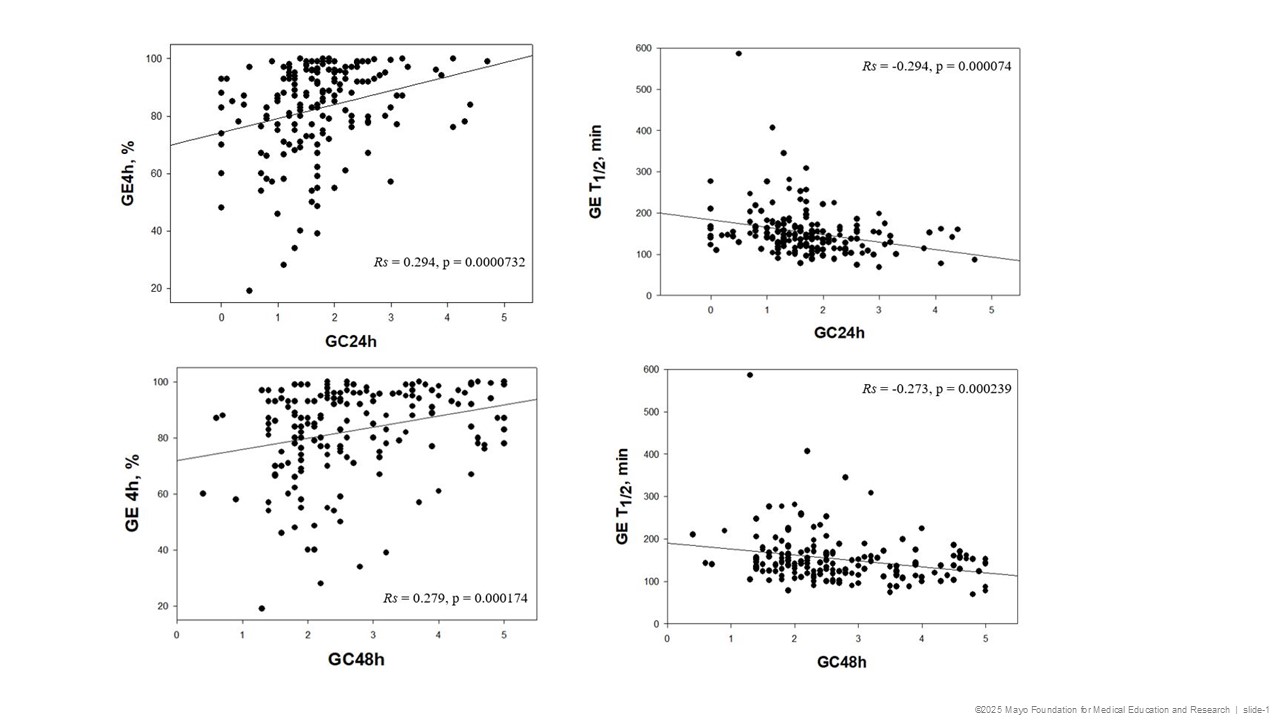
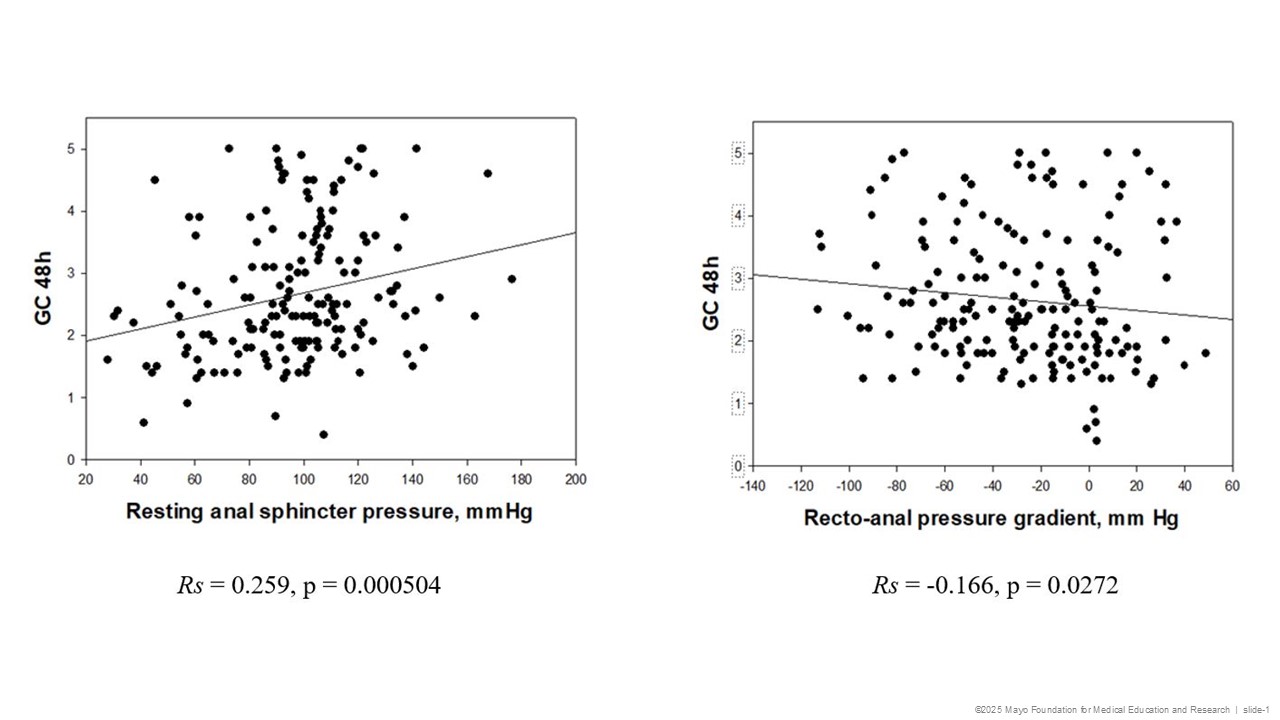
Nada Abdelnaem, MD, John Damianos, MD, Michael Camilleri, MD, DSc Mayo Clinic, Rochester, MN Introduction: Upper and lower gastrointestinal (GI) dysfunctions frequently coexist. Potential mechanisms include gastrocolonic or cologastric neural reflexes. The relationship between colonic transit (CT), dyssynergic defecation (DD), gastric emptying (GE) and gastric accommodation (GA) remains largely unexplored. Aims: To assess the prevalence of impaired GA and delayed GE among patients with lower gastrointestinal dysfunction, and to evaluate relationships between CT or DD with impaired GA and delayed GE. Methods: We conducted an IRB-approved retrospective review of adult patients at Mayo Clinic (2005–2025) with documented slow CT or DD (based respectively on scintigraphic CT, and high resolution anorectal manometry [ARM] and balloon expulsion [BE]) who underwent measurement of GA by 99mTc-SPECT imaging following 300mL Ensure®, and GE of a 99mTc-labeled, 320-kcal, 30% fat egg meal by scintigraphy. Slow CT was defined relative to 220 healthy controls: geometric center (GC) at 48h < 2.1 for males and < 1.9 for females. DD was based on resting anal pressure (RAP), rectoanal pressure gradient (RAPG), and % anal relaxation during the ARM test. GA was assessed relative to 10-90%ile from 354 healthy controls [ratio of postprandial to fasting volume < 2.62 (reduced), >3.85 (increased) GA], and delayed GE relative to data from 319 healthy participants (GE% < 75 at 4h). Correlations were assessed using Spearman Rank test. Results: Reduced GA was found in 23.7% patients with DD and 26.7% with slow CT; increased GA was observed in 30.1% and 24.4%, respectively. Delayed GE was present in 20.5% patients with DD and 35.6% with slow CT. There were moderate associations for CT: GC48 positively with GE% 4h (Rs=0.279, p < 0.001) and negatively with GE T1/2 (Rs= -0.273, p < 0.001) suggesting slow CT retards GE. Similarly, GC24 correlated with GE% 4h (Rs=0.294, p< 0.001) and GE T1/2 (Rs= -0.294, p< 0.001). GC48 was moderately correlated with RAP (Rs=0.259, p< 0.001) and negatively with the RAPG (Rs= -0.166, p=0.027). No significant correlations were observed between CT and GA. Discussion: Slow CT is associated with slower GE, suggesting cologastric reflex inhibition. The high prevalence of impaired GA and delayed GE in slow CT and DD underscores the need for a comprehensive diagnostic approach in the presence of both chronic constipation and upper GI symptoms. The lack of correlation between slow CT and GA argues against cologastric interactions in impaired GA.
Figure: Figure 1. Left Panel: Spearman Rank Order Correlations for the associations between colonic transit parameters GC 24h and GC 48h and GE% at 4h showing moderate statistically significant positive correlations (p < 0.050). Right Panel: Spearman Rank Order Correlations for the associations between colonic transit parameters GC 24h and GC 48h and GE T1/2 showing moderate statistically significant negative correlations (p < 0.050).
Figure: Figure 2. Left Panel: Spearman Rank Order Correlation for the association between resting anal sphincter pressure and GC 48h showing a moderate statistically significant positive correlation (p < 0.050). Right Panel: Spearman Rank Order Correlation for the association between recto-anal pressure gradient and GC 48h showing a moderate statistically significant negative correlation (p < 0.050).
Nada Abdelnaem, MD, John Damianos, MD, Michael Camilleri, MD, DSc. P4563 - Cologastric Inhibition: Association Between Lower and Upper Gastrointestinal Dysfunction, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.