
Tuesday Poster Session
Category: Colon
 photo")
Andrew L. Petrou, MD (he/him/his)
Brown University / Rhode Island Hospital
Providence, RI
Omental infarction is a rare condition that occurs when there is tissue death of the omentum, the fatty layer of tissue that covers the intestines and other abdominal organs. This condition occurs when there is a disruption in the blood flow. Omental infarction presents with acute abdominal pain and can oftentimes be mistaken for other causes of abdominal pain. Here we describe a case of a patient who developed an omental infarction following polypectomy of a large cecal polyp the day prior to her presentation.
Case Description/
Methods:
A 58-year-old female with past medical history of hypertension, presents to the emergency department (ED) with acute-onset abdominal pain one day following a screening colonoscopy. The pain started several hours following her colonoscopy. During the colonoscopy she had one 2 mm tubular adenoma (TA) removed in the transverse colon and one 20 mm TA removed in the cecum using injection-lift and piecemeal endoscopic mucosal resection with a cold snare. Brief external pressure was applied to assist with cecal intubation, but otherwise the procedure was uncomplicated and the patient was discharged home in baseline health. On physical examination in the ED, she was afebrile, her blood pressure was 139/83, and heart rate 70 beats per minute. Abdominal examination was notable for tenderness to palpation in the right-lower quadrant. A computed tomography (CT) of the abdomen and pelvis with contrast demonstrated clips located in the cecum and inflammatory stranding dorsal to the right colon suggesting omental infarction. There was no evidence of perforation on CT scan, nor inflammatory changes adjacent to the cecal polypectomy site. The patient was ultimately discharged home with NSAID analgesics and her pain resolved within several days.
Discussion:
Omental infarction is an uncommon complication following colonoscopy, and its exact cause is unknown. During a polypectomy, manipulation of surrounding structures may inadvertently affect the omental perfusion; particularly if excess traction is placed on the colon. It is unclear if colonic looping or the actual polypectomy including submucosal lifting or hemostatic clips, contributed to the omental ischemia. Post-polypectomy syndrome would show inflammatory findings on imaging, though more often at the site or adjacent to the polypectomy site; which was not observed in this case. Like many cases of omental infarction, this patient made a full recovery with supportive care. 
Figure: Figure 1. Clips within the cecum on CT Abdomen. B. Inflammatory stranding dorsal to the right colon demonstrating omental infarction on CT Abdomen.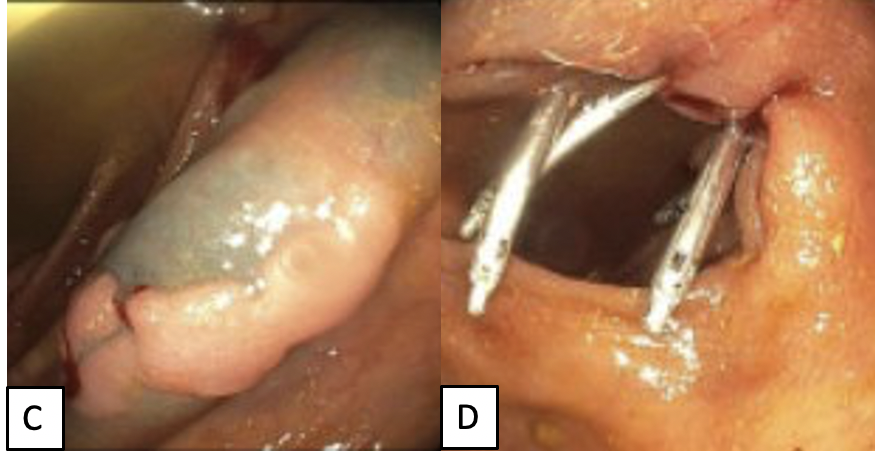
Figure: Figure 2. C. Polyp after injection lift prior to piecemeal removal with cold snare. D. Post-polypectomy site with clips in place.
Disclosures:
Andrew Petrou indicated no relevant financial relationships.
Audrey Ballard indicated no relevant financial relationships.
Grace Wilgucki indicated no relevant financial relationships.
Breton Roussel: Johnson and Johnson – Speakers Bureau. Phathom Pharmaceuticals – Speakers Bureau.
Andrew L. Petrou, MD1, Audrey Ballard, MD1, Grace Wilgucki, DO2, Breton Roussel, MD3. P4607 - Fatty Surprise: A Rare Case of Omental Infarction Following Polypectomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.