
Tuesday Poster Session
Category: Colon
Matthew Orosa, DO
Riverside University Health System
Moreno Valley, California
A cholecystocolonic fistula (CCF) is an abnormal connection between the gallbladder and the colon, typically resulting from chronic inflammation of the gallbladder caused by gallstones. CCFs are less common than other cholecystoenteric fistulae, with cholecystoduodenal fistulae being more frequent. Cholecystocolonic fistulae occur in 0.06%-0.14% of patients with biliary disease. Furthermore, mechanical obstruction linked to these types of fistulae are rare, with only a few cases documented in the literature. This case aims to highlight this rare association, and clinicians should be made aware of this clinical entity.
Case Description/
Methods:
A 59-year-old female with type 2 diabetes and hypertension presented to the hospital with 2 days of abdominal pain, vomiting, and obstipation. On physical examination, abdominal tenderness was noted, and labs revealed a leukocytosis of 19.3. Computed tomography scan revealed a patent fistulous connection between the gallbladder and ascending colon at the hepatic flexure. A 2.1 x 1.1 cm gallstone was identified in the sigmoid colon, accompanied by a large bowel dilation measuring up to 9.5 cm, raising concerns for mechanical bowel obstruction. Attempts to remove the stone via colonoscopy with hot snare, retrieval basket, and electrohydraulic lithotripsy were unsuccessful, thus exploratory laparotomy was done. Most cases of gallstone ileus involve an enterotomy (incision in the bowel to remove the stone), which may lead to complications such as infection and dehiscence. In this case, the stone was manually squeezed out through the rectum during surgery, allowing the patient to avoid the need for an enterotomy. Prior to discharge, the patient had regular bowel movements and was able to tolerate a full diet without any issues, indicating a stable and improving condition.
Discussion:
Mechanical large bowel obstructions resulting from CCFs are a rare occurrence. The underlying pathophysiology involves chronic inflammation of the gallbladder secondary to gallstones. Other recognized causes include gallbladder malignancies, previous gastric surgeries, and abdominal trauma. This case also demonstrated the successful management of the gallstone without the need for an enterotomy, which is typically required in such cases. Ischemia and sepsis are severe complications that may arise from this type of obstruction. Therefore, healthcare providers must be vigilant to diagnose and treat the condition promptly.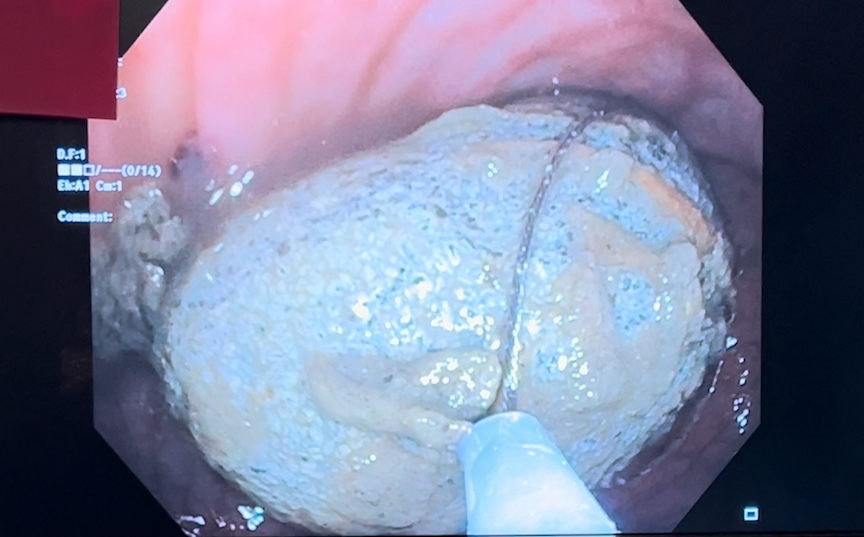
Figure: Fistula formation between gallbladder and colon.
Figure: Presence of a gallstone in the colonic lumen.
Disclosures:
Matthew Orosa indicated no relevant financial relationships.
Mena Saad indicated no relevant financial relationships.
Andrew Chang indicated no relevant financial relationships.
Matthew Orosa, DO1, Mena Saad, DO1, Andrew Chang, MD2. P4669 - Mechanical Large Bowel Obstruction in a Patient Found to Have a Cholecystocolonic Fistula, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.